

A Prognostic Gene Expression Signature in the Molecular Classification of Chemotherapy-naïve Urothelial Cancer is Predictive of Clinical Outcomes from Neoadjuvant Chemotherapy: A Phase 2 Trial of Dose-dense Methotrexate, Vinblastine, Doxorubicin, and Cisplatin with Bevacizumab in Urothelial Cancer
- PMID: 26343003
- PMCID: PMC4775435
- DOI: 10.1016/j.eururo.2015.08.034
A Prognostic Gene Expression Signature in the Molecular Classification of Chemotherapy-naïve Urothelial Cancer is Predictive of Clinical Outcomes from Neoadjuvant Chemotherapy: A Phase 2 Trial of Dose-dense Methotrexate, Vinblastine, Doxorubicin, and Cisplatin with Bevacizumab in Urothelial Cancer
Abstract
Background: Gene expression profiling (GEP) suggests there are three subtypes of muscle-invasive urothelial cancer (UC): basal, which has the worst prognosis; p53-like; and luminal. We hypothesized that GEP of transurethral resection (TUR) and cystectomy specimens would predict subtypes that could benefit from chemotherapy.
Objective: To explore clinical outcomes for patients treated with dose-dense (DD) methotrexate, vinblastine, doxorubicin, and cisplatin (MVAC) and bevacizumab (B) and the impact of UC subtype.
Design, setting, and participants: Sixty patients enrolled in a neoadjuvant trial of four cycles of DDMVAC + B between 2007 and 2010. TUR and cystectomy specimens for GEP were available from 38 and 23 patients, respectively, and from an additional confirmation cohort of 49 patients treated with perioperative MVAC.
Outcome measurements and statistical analysis: Relationships with outcomes were analyzed using multivariable Cox regression and log-rank tests.
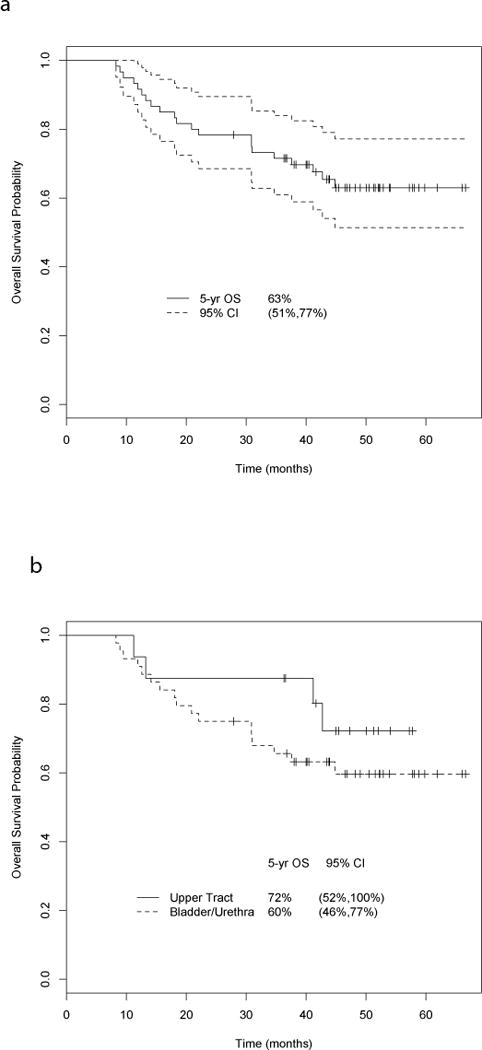
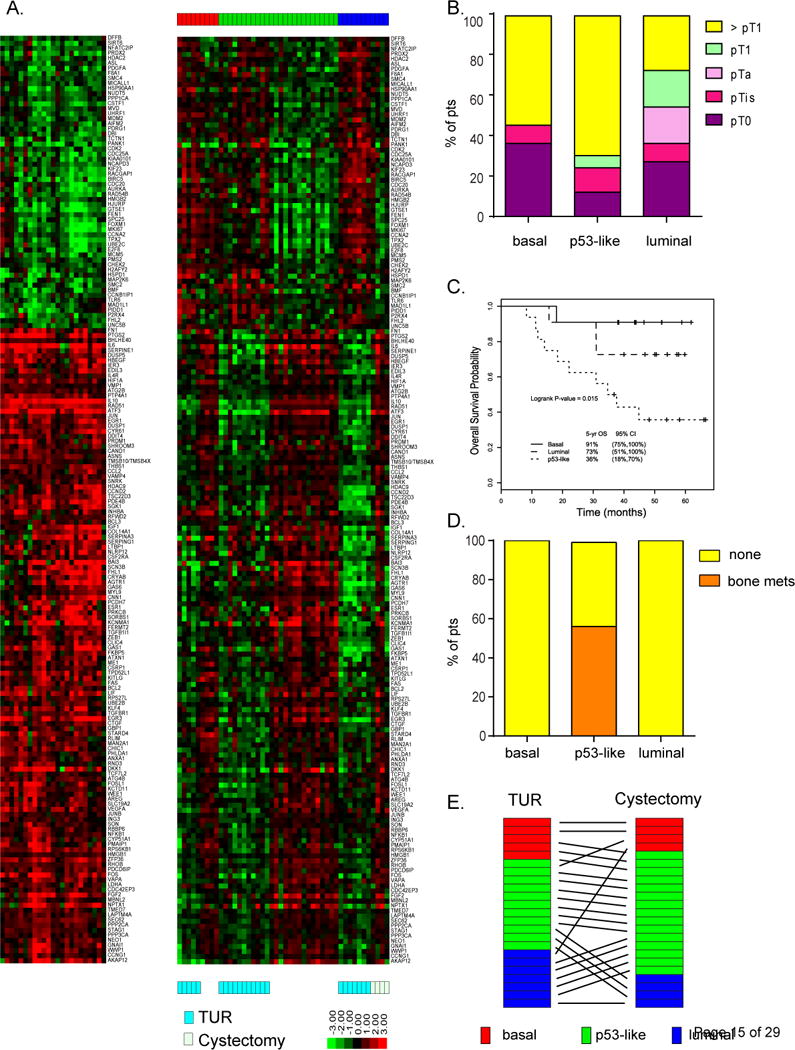
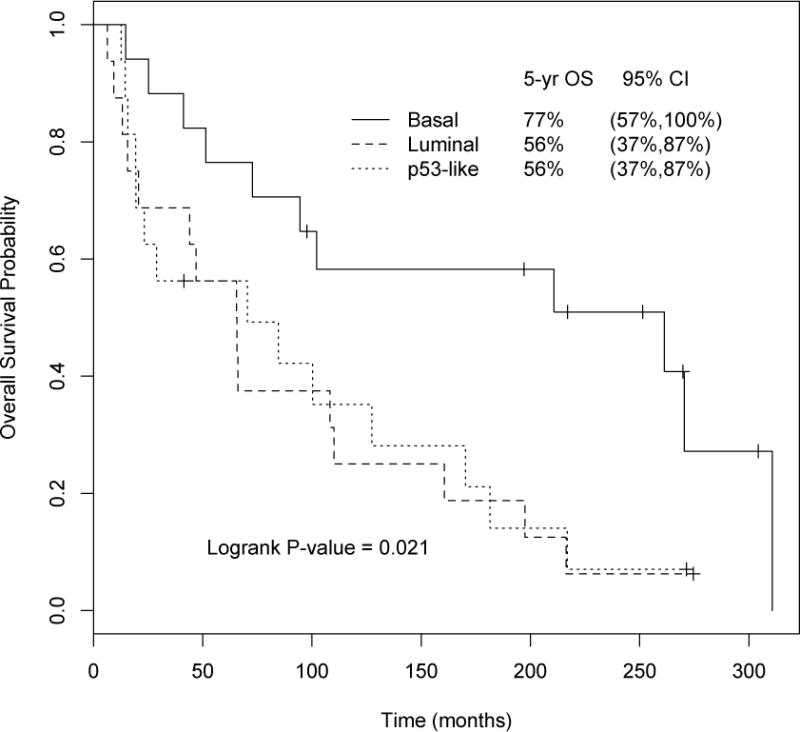
Results and limitations: Chemotherapy was active, with pT0N0 and ≤pT1N0 downstaging rates of 38% and 53%, respectively, and 5-yr overall survival (OS) of 63%. Bevacizumab had no appreciable impact on outcomes. Basal tumors had improved survival compared to luminal and p53-like tumors (5-yr OS 91%, 73%, and 36%, log-rank p=0.015), with similar findings on multivariate analysis. Bone metastases within 2 yr were exclusively associated with the p53-like subtype (p53-like 100%, luminal 0%, basal 0%; p ≤ 0.001). Tumors enriched with the p53-like subtype at cystectomy suggested chemoresistance for this subtype. A separate cohort treated with perioperative MVAC confirmed the UC subtype survival benefit (5-yr OS 77% for basal, 56% for luminal, and 56% for p53-like; p=0.021). Limitations include the small number of pretreatment specimens with sufficient tissue for GEP.
Conclusion: GEP was predictive of clinical UC outcomes. The basal subtype was associated with better survival, and the p53-like subtype was associated with bone metastases and chemoresistant disease.
Patient summary: We can no longer think of urothelial cancer as a single disease. Gene expression profiling identifies subtypes of urothelial cancer that differ in their natural history and sensitivity to chemotherapy.
Keywords: Basal; Bevacizumab; Dose-dense methotrexate cisplatin; Gene expression profiling; Luminal; Neoadjuvant; Subtype; Urothelial cancer; p53.
Copyright © 2015 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
The Neoadjuvant Paradigm for Development of Systemic Therapy and Precision Medicine for Bladder Cancer.Eur Urol. 2016 May;69(5):863-5. doi: 10.1016/j.eururo.2015.09.018. Epub 2015 Sep 26. Eur Urol. 2016. PMID: 26414768 No abstract available.
References
-
- Grossman HB, Natale RB, Tangen CM, et al. Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. N Engl J Med. 2003;349:859–66. - PubMed
-
- Sternberg CN, Bellmunt J, Sonpavde G, et al. ICUD-EAU International Consultation on Bladder Cancer 2012: chemotherapy for urothelial carcinoma—neoadjuvant and adjuvant settings. Eur Urol. 2013;63:58–66. - PubMed
-
- Inoue K, Slaton JW, Karashima T, et al. The prognostic value of angiogenesis factor expression for predicting recurrence and metastasis of bladder cancer after neoadjuvant chemotherapy and radical cystectomy. Clin Cancer Res. 2000;6:4866–73. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
