

Retinal Architecture in RGS9- and R9AP-Associated Retinal Dysfunction (Bradyopsia)
- PMID: 26343007
- PMCID: PMC4653116
- DOI: 10.1016/j.ajo.2015.08.032
Retinal Architecture in RGS9- and R9AP-Associated Retinal Dysfunction (Bradyopsia)
Abstract
Purpose: To characterize photoreceptor structure and mosaic integrity in subjects with RGS9- and R9AP-associated retinal dysfunction (bradyopsia) and compare to previous observations in other cone dysfunction disorders such as oligocone trichromacy.
Design: Observational case series.
Methods: setting: Moorfields Eye Hospital (United Kingdom) and Medical College Wisconsin (USA).
Study population: Six eyes of 3 subjects with disease-causing variants in RGS9 or R9AP.
Main outcome measures: Detailed retinal imaging using spectral-domain optical coherence tomography and confocal adaptive-optics scanning light ophthalmoscopy.
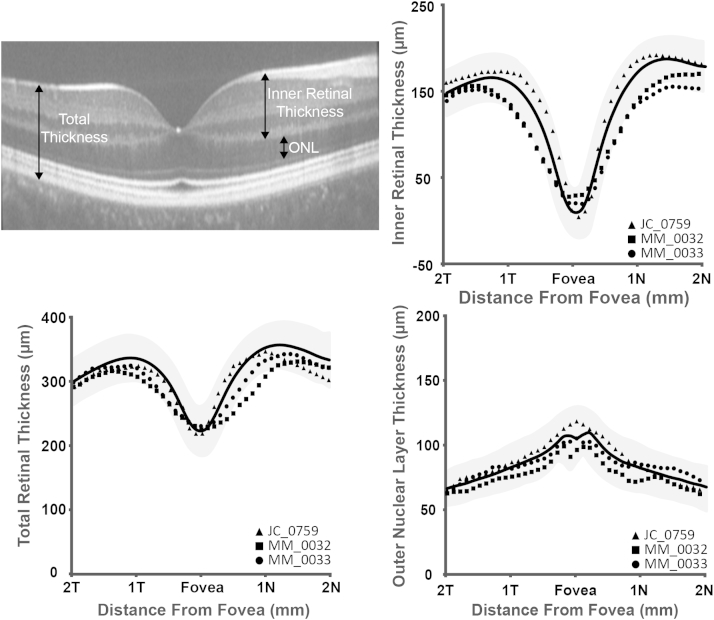
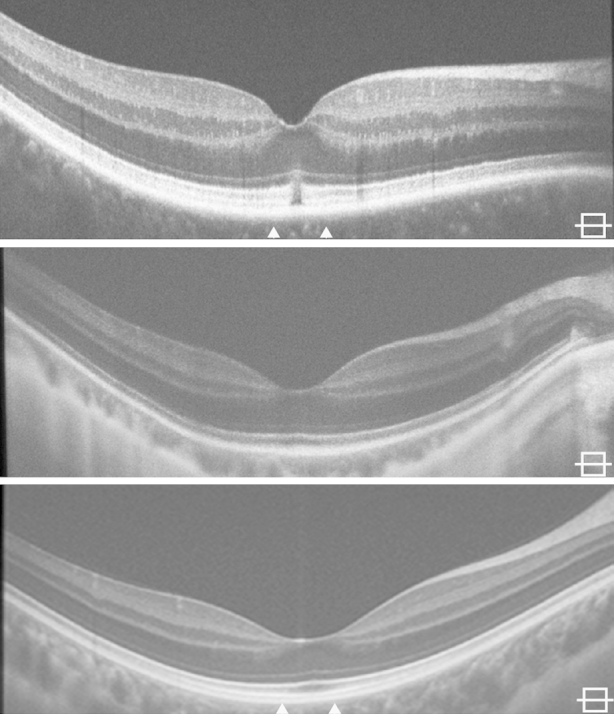
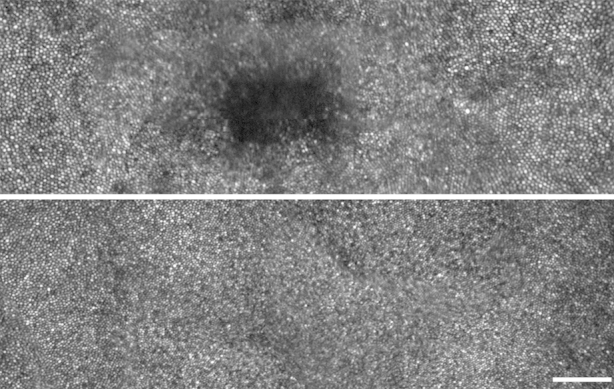
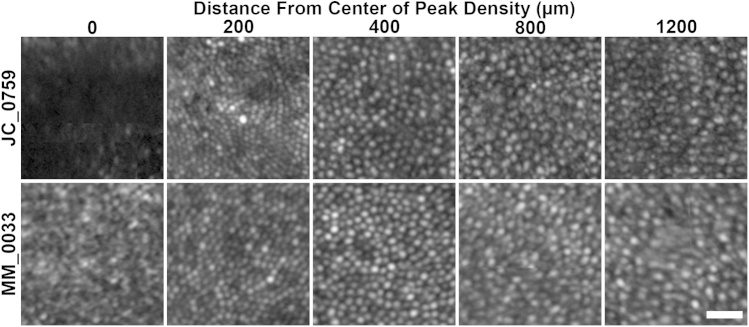
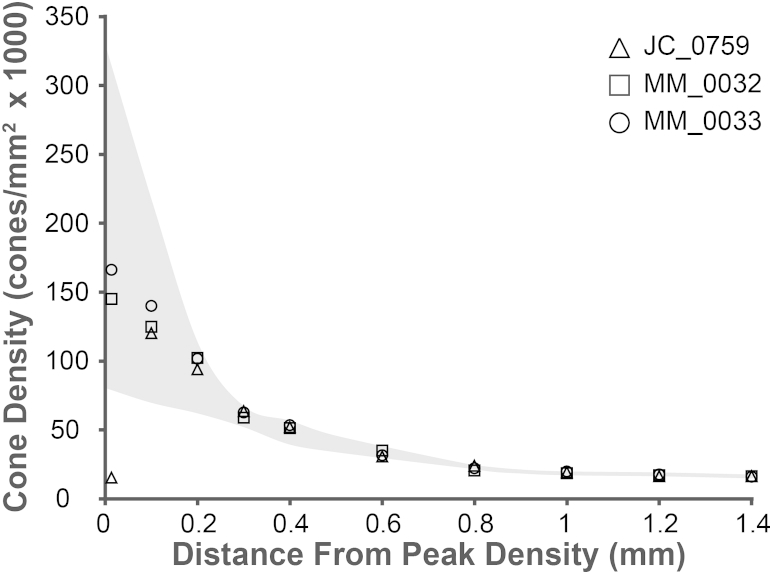
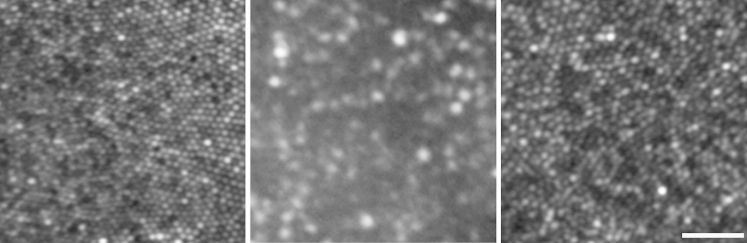
Results: Cone density at 100 μm from foveal center ranged from 123 132 cones/mm(2) to 140 013 cones/mm(2). Cone density ranged from 30 573 to 34 876 cones/mm(2) by 600 μm from center and from 15 987 to 16,253 cones/mm(2) by 1400 μm from center, in keeping with data from normal subjects. Adaptive-optics imaging identified a small, focal hyporeflective lesion at the foveal center in both eyes of the subject with RGS9-associated disease, corresponding to a discrete outer retinal defect also observed on spectral-domain optical coherence tomography; however, the photoreceptor mosaic remained intact at all other observed eccentricities.
Conclusions: Bradyopsia and oligocone trichromacy share common clinical symptoms and cannot be discerned on standard clinical findings alone. Adaptive-optics imaging previously demonstrated a sparse mosaic of normal wave-guiding cones remaining at the fovea, with no visible structure outside the central fovea in oligocone trichromacy. In contrast, the subjects presented in this study with molecularly confirmed bradyopsia had a relatively intact and structurally normal photoreceptor mosaic, allowing the distinction between these disorders based on the cellular phenotype and suggesting different pathomechanisms.
Copyright © 2015 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Integrity of the cone photoreceptor mosaic in oligocone trichromacy.Invest Ophthalmol Vis Sci. 2011 Jul 1;52(7):4757-64. doi: 10.1167/iovs.10-6659. Invest Ophthalmol Vis Sci. 2011. PMID: 21436275 Free PMC article.
-
Novel mutations and electrophysiologic findings in RGS9- and R9AP-associated retinal dysfunction (Bradyopsia).Ophthalmology. 2010 Jan;117(1):120-127.e1. doi: 10.1016/j.ophtha.2009.06.011. Epub 2009 Oct 8. Ophthalmology. 2010. PMID: 19818506
-
Cone abnormalities in fundus albipunctatus associated with RDH5 mutations assessed using adaptive optics scanning laser ophthalmoscopy.Am J Ophthalmol. 2014 Mar;157(3):558-70.e1-4. doi: 10.1016/j.ajo.2013.10.021. Epub 2013 Nov 16. Am J Ophthalmol. 2014. PMID: 24246574
-
Cones in ageing and harsh environments: the neural economy hypothesis.Ophthalmic Physiol Opt. 2020 Mar;40(2):88-116. doi: 10.1111/opo.12670. Epub 2020 Feb 4. Ophthalmic Physiol Opt. 2020. PMID: 32017191 Free PMC article. Review.
-
Dysflective Cones.Adv Exp Med Biol. 2019;1185:133-137. doi: 10.1007/978-3-030-27378-1_22. Adv Exp Med Biol. 2019. PMID: 31884601 Free PMC article. Review.
Cited by
-
From Cellular to Metabolic: Advances in Imaging of Inherited Retinal Diseases.Diagnostics (Basel). 2024 Dec 26;15(1):28. doi: 10.3390/diagnostics15010028. Diagnostics (Basel). 2024. PMID: 39795556 Free PMC article. Review.
-
Adaptive optics imaging of inherited retinal diseases.Br J Ophthalmol. 2018 Aug;102(8):1028-1035. doi: 10.1136/bjophthalmol-2017-311328. Epub 2017 Nov 15. Br J Ophthalmol. 2018. PMID: 29141905 Free PMC article. Review.
-
Impact of Reference Center Choice on Adaptive Optics Imaging Cone Mosaic Analysis.Invest Ophthalmol Vis Sci. 2022 Apr 1;63(4):12. doi: 10.1167/iovs.63.4.12. Invest Ophthalmol Vis Sci. 2022. PMID: 35446344 Free PMC article.
-
Retinal findings in a patient of French ancestry with CABP4-related retinal disease.Doc Ophthalmol. 2018 Apr;136(2):135-143. doi: 10.1007/s10633-018-9629-y. Epub 2018 Mar 10. Doc Ophthalmol. 2018. PMID: 29525873
-
Monogenic Retinal Diseases Associated With Genes Encoding Phototransduction Proteins: A Review.Clin Exp Ophthalmol. 2025 Apr;53(3):260-280. doi: 10.1111/ceo.14511. Epub 2025 Feb 27. Clin Exp Ophthalmol. 2025. PMID: 40013354 Free PMC article. Review.
References
-
- Kooijman A.C., Houtman A., Damhof A., van Engelen J.P. Prolonged electro-retinal response suppression (PERRS) in patients with stationary subnormal visual acuity and photophobia. Doc Ophthalmol. 1991;78(3-4):245–254. - PubMed
-
- Nishiguchi K.M., Sandberg M.A., Kooijman A.C. Defects in RGS9 or its anchor protein R9AP in patients with slow photoreceptor deactivation. Nature. 2004;427(6969):75–78. - PubMed
-
- Michaelides M., Li Z., Rana N.A. Novel mutations and electrophysiologic findings in RGS9- and R9AP-associated retinal dysfunction (Bradyopsia) Ophthalmology. 2010;117(1):120–127.e1. - PubMed
-
- Hartong D.T., Pott J.W., Kooijman A.C. Six patients with bradyopsia (slow vision): clinical features and course of the disease. Ophthalmology. 2007;114(12):2323–2331. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
