

Clinical determinants of early parasitological response to ACTs in African patients with uncomplicated falciparum malaria: a literature review and meta-analysis of individual patient data
- PMID: 26343145
- PMCID: PMC4561425
- DOI: 10.1186/s12916-015-0445-x
Clinical determinants of early parasitological response to ACTs in African patients with uncomplicated falciparum malaria: a literature review and meta-analysis of individual patient data
Abstract
Background: Artemisinin-resistant Plasmodium falciparum has emerged in the Greater Mekong sub-region and poses a major global public health threat. Slow parasite clearance is a key clinical manifestation of reduced susceptibility to artemisinin. This study was designed to establish the baseline values for clearance in patients from Sub-Saharan African countries with uncomplicated malaria treated with artemisinin-based combination therapies (ACTs).
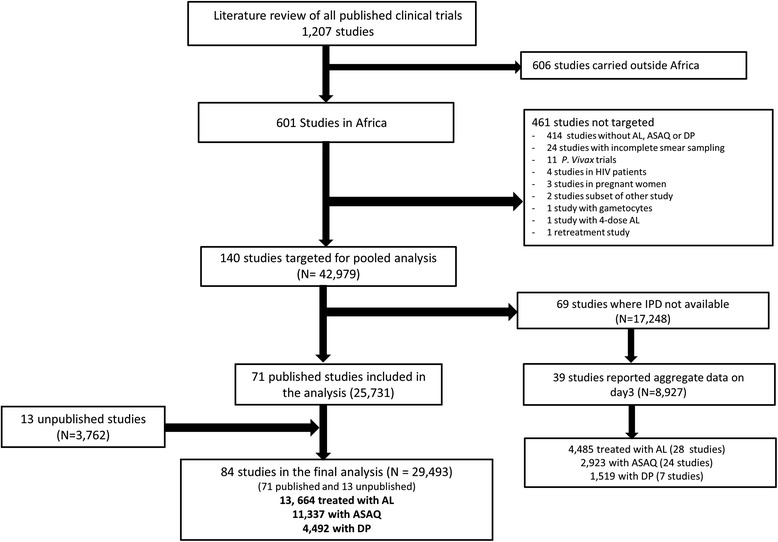
Methods: A literature review in PubMed was conducted in March 2013 to identify all prospective clinical trials (uncontrolled trials, controlled trials and randomized controlled trials), including ACTs conducted in Sub-Saharan Africa, between 1960 and 2012. Individual patient data from these studies were shared with the WorldWide Antimalarial Resistance Network (WWARN) and pooled using an a priori statistical analytical plan. Factors affecting early parasitological response were investigated using logistic regression with study sites fitted as a random effect. The risk of bias in included studies was evaluated based on study design, methodology and missing data.
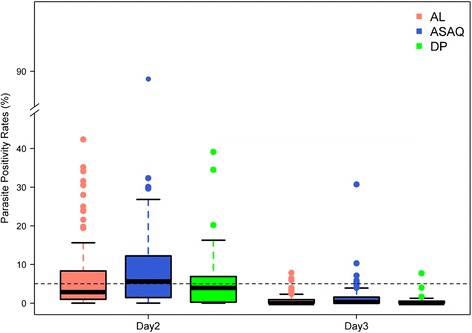
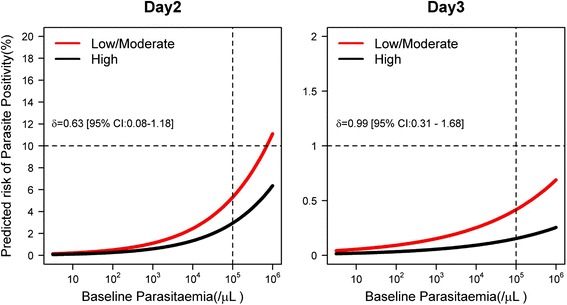
Results: In total, 29,493 patients from 84 clinical trials were included in the analysis, treated with artemether-lumefantrine (n = 13,664), artesunate-amodiaquine (n = 11,337) and dihydroartemisinin-piperaquine (n = 4,492). The overall parasite clearance rate was rapid. The parasite positivity rate (PPR) decreased from 59.7 % (95 % CI: 54.5-64.9) on day 1 to 6.7 % (95 % CI: 4.8-8.7) on day 2 and 0.9 % (95 % CI: 0.5-1.2) on day 3. The 95th percentile of observed day 3 PPR was 5.3 %. Independent risk factors predictive of day 3 positivity were: high baseline parasitaemia (adjusted odds ratio (AOR) = 1.16 (95 % CI: 1.08-1.25); per 2-fold increase in parasite density, P <0.001); fever (>37.5 °C) (AOR = 1.50 (95 % CI: 1.06-2.13), P = 0.022); severe anaemia (AOR = 2.04 (95 % CI: 1.21-3.44), P = 0.008); areas of low/moderate transmission setting (AOR = 2.71 (95 % CI: 1.38-5.36), P = 0.004); and treatment with the loose formulation of artesunate-amodiaquine (AOR = 2.27 (95 % CI: 1.14-4.51), P = 0.020, compared to dihydroartemisinin-piperaquine).
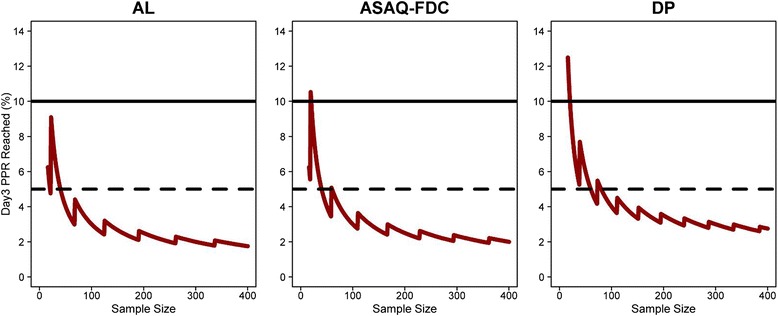
Conclusions: The three ACTs assessed in this analysis continue to achieve rapid early parasitological clearance across the sites assessed in Sub-Saharan Africa. A threshold of 5 % day 3 parasite positivity from a minimum sample size of 50 patients provides a more sensitive benchmark in Sub-Saharan Africa compared to the current recommended threshold of 10 % to trigger further investigation of artemisinin susceptibility.
Figures
Comment in
-
Parasite clearance after malaria therapy: staying a step ahead of drug resistance.BMC Med. 2015 Oct 2;13:251. doi: 10.1186/s12916-015-0486-1. BMC Med. 2015. PMID: 26429335 Free PMC article.
References
-
- World Health Organization (WHO) World malaria report 2014. Geneva: WHO; 2014.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
