

HIV infection induces structural and functional changes in high density lipoproteins
- PMID: 26343868
- PMCID: PMC4609619
- DOI: 10.1016/j.atherosclerosis.2015.08.036
HIV infection induces structural and functional changes in high density lipoproteins
Abstract
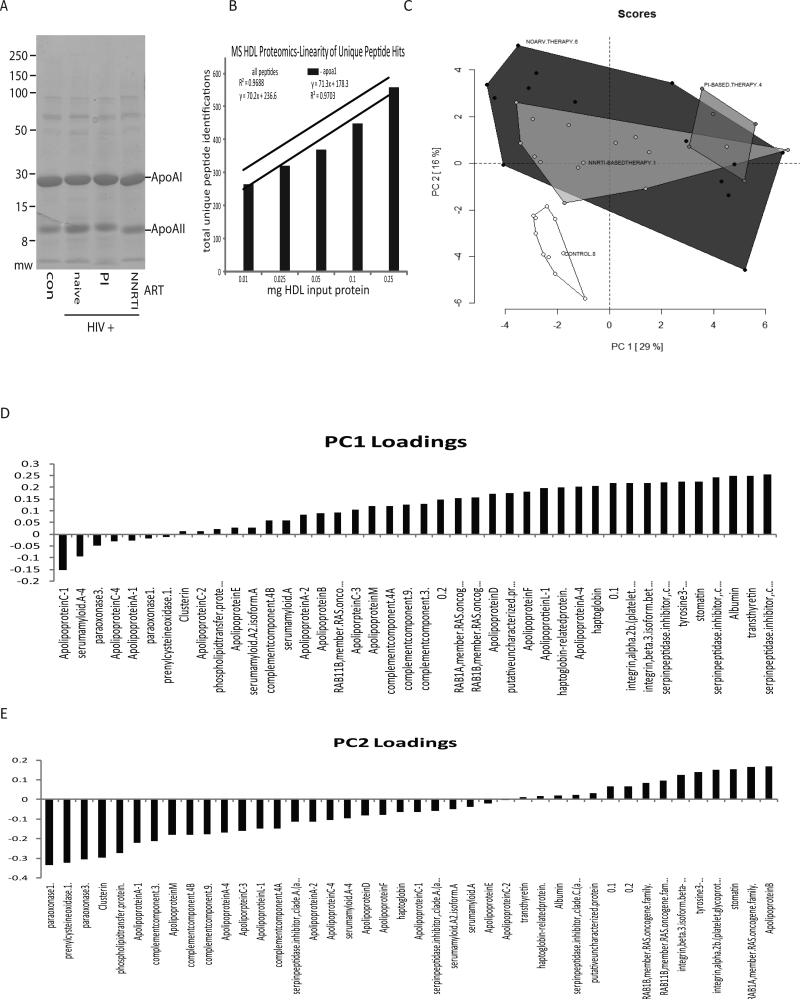
Background and aims: Coronary artery disease is a growing clinical problem in HIV-infected subjects. The increased risk of coronary events in this population has been linked to low levels of HDL, but the effects of HIV infection and anti-retroviral treatment (ART) on HDL structure and function remain unknown. Here, we aimed to determine the composition and function of HDL particles isolated from ART-naive and ART-positive HIV-infected patients.
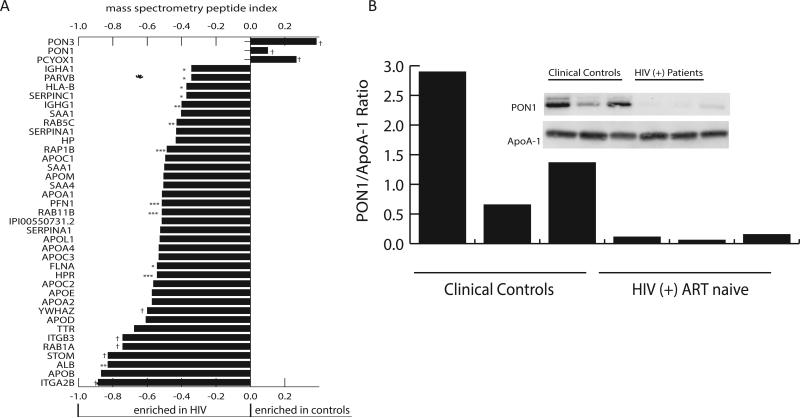
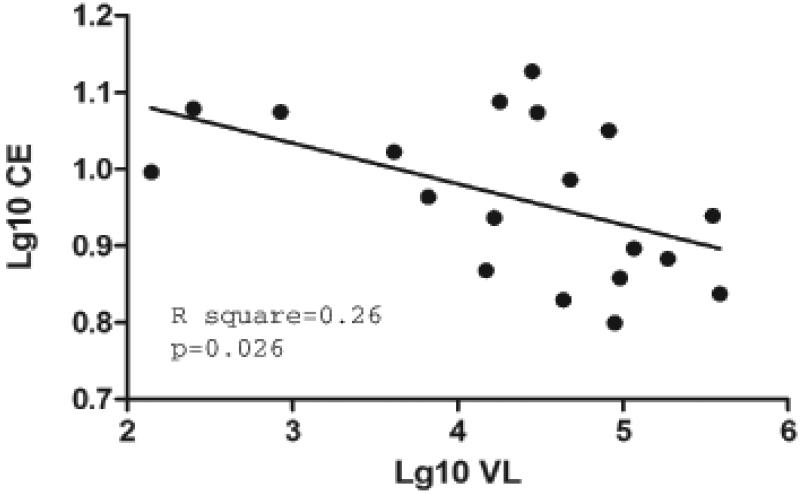
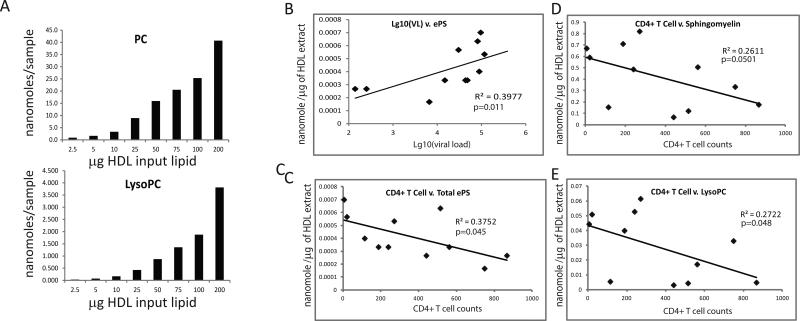
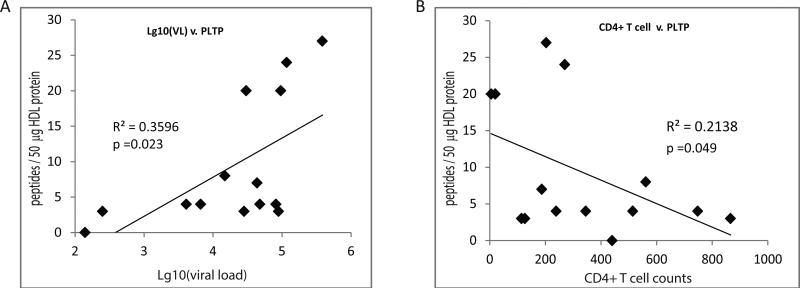
Methods and results: Proteomic profiling revealed decreased levels of paraoxonase (PON) 1 and PON 3 in HDL from HIV patients relative to HDL from uninfected controls (p < 0.0001), and PON activity of HDL from control group (0.13 ± 0.01 U/μl) was significantly higher than PON activity of HDL from HIV-infected untreated subjects (0.12 ± 0.01 U/μl, p = 0.0035), subjects treated with non-nucleoside reverse transcriptase inhibitor (NNRTI)-based therapy (0.11 ± 0.01 U/μl, p < 0.0001), subjects treated with protease inhibitor (PI)-based therapy with detectable viral load (0.11 ± 0.01 U/μl, p < 0.0001), and PI-treated patients with undetectable viral load (0.12 ± 0.01 U/μl, p = 0.0164). Lipidomic profiling uncovered a negative correlation between CD4 T cell counts and particle sphingomyelin, lyso-phosphatidylcholine and ether-linked phosphatidylserine content in the ART-naive (R(2) = 0.2611, p < 0.05; R(2) = 0.2722, p < 0.05; and R(2) = 0.3977, p < 0.05, respectively) but not treated HIV-infected subjects. Functional analysis demonstrated a negative correlation between cholesterol efflux capacity of HDL and viral load in the ART-naive HIV-infected group (R(2) = 0.26, p = 0.026).
Conclusions: Taken together, these results indicate that HIV infection associates with a number of both protein and lipid compositional changes in HDL particles. Moreover, HIV infection affects cholesterol efflux function of HDL, thus contributing to an increased risk of atherosclerosis in this patient population.
Keywords: Anti-retroviral treatment; Atherosclerosis; Cholesterol efflux; HDL; HIV; Lipidomics; PON; Proteomics.
Copyright © 2015 Elsevier Ireland Ltd. All rights reserved.
Figures
References
-
- Escaut L, Monsuez JJ, Chironi G, et al. Coronary artery disease in HIV infected patients. Intensive Care Med. 2003;29:969–973. - PubMed
-
- Lang S, Mary-Krause M, Cotte L, et al. Increased risk of myocardial infarction in HIV-infected patients in France, relative to the general population. AIDS. 2010;24:1228–1230. - PubMed
-
- Kwong GP, Ghani AC, Rode RA, et al. Comparison of the risks of atherosclerotic events versus death from other causes associated with antiretroviral use. AIDS. 2006;20:1941–1950. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
