

Comparative diagnostic performance of volumetric laser endomicroscopy and confocal laser endomicroscopy in the detection of dysplasia associated with Barrett's esophagus
- PMID: 26344884
- PMCID: PMC5554864
- DOI: 10.1016/j.gie.2015.08.050
Comparative diagnostic performance of volumetric laser endomicroscopy and confocal laser endomicroscopy in the detection of dysplasia associated with Barrett's esophagus
Abstract
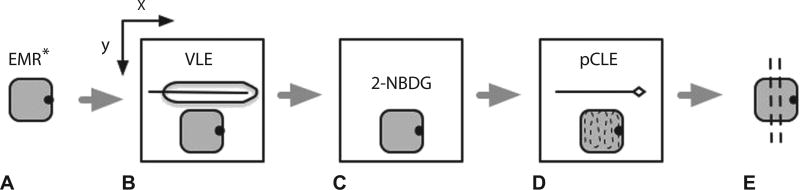
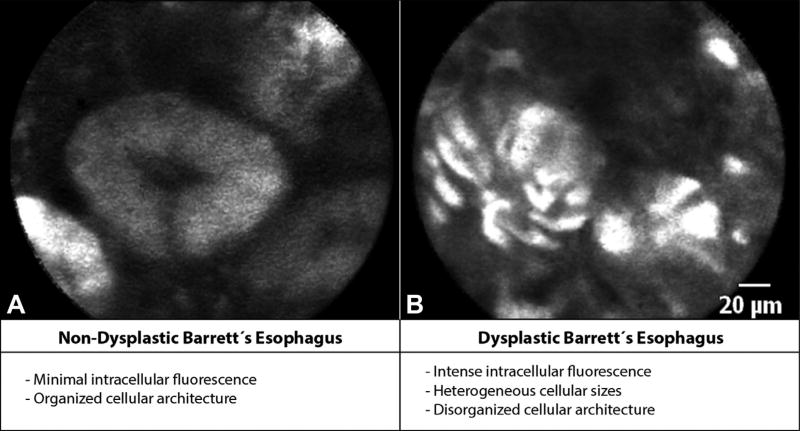
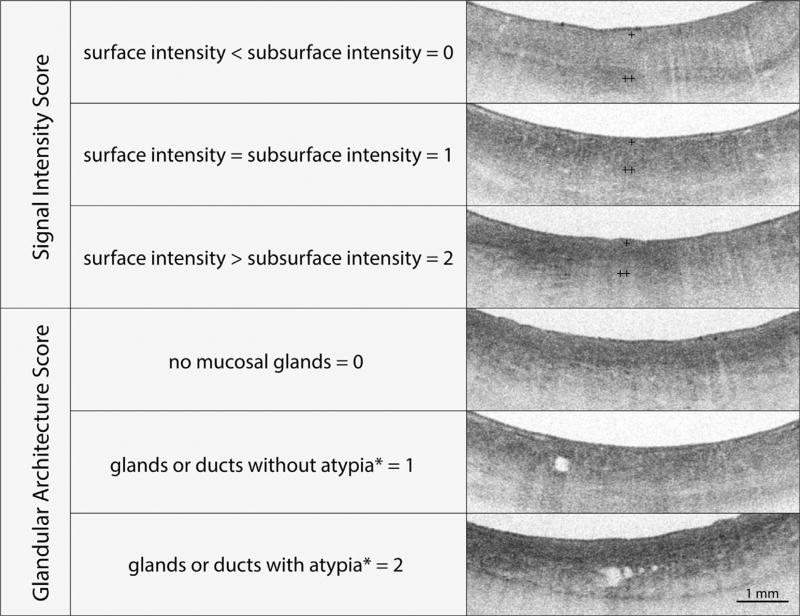
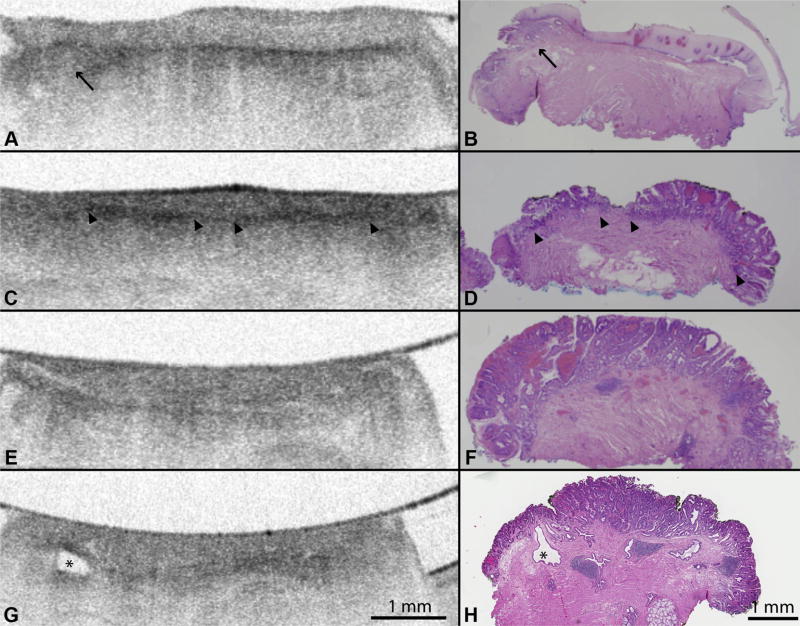
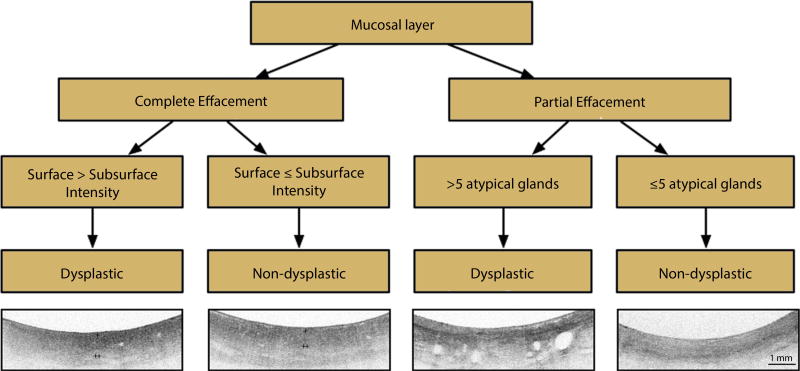
Background and aims: Probe-based confocal laser endomicroscopy (pCLE) and volumetric laser endomicroscopy (VLE) (also known as frequency domain optical coherence tomography) are advanced endoscopic imaging modalities that may be useful in the diagnosis of dysplasia associated with Barrett's esophagus (BE). We performed pCLE examination in ex-vivo EMR specimens and compared the diagnostic performance of using the current VLE scoring index (previously established as OCT-SI) and a novel VLE diagnostic algorithm (VLE-DA) for the detection of dysplasia.
Methods: A total of 27 patients with BE enrolled in a surveillance program at a tertiary-care center underwent 50 clinically indicated EMRs that were imaged with VLE and pCLE and classified into neoplastic (N = 34; high-grade dysplasia, intramucosal adenocarcinoma) and nonneoplastic (N = 16; low-grade dysplasia, nondysplastic BE), based on histology. Image datasets (VLE, N = 50; pCLE, N = 50) were rated by 3 gastroenterologists trained in the established diagnostic criteria for each imaging modality as well as a new diagnostic algorithm for VLE derived from a training set that demonstrated association of specific VLE features with neoplasia. Sensitivity, specificity, and diagnostic accuracy were assessed for each imaging modality and diagnostic criteria.
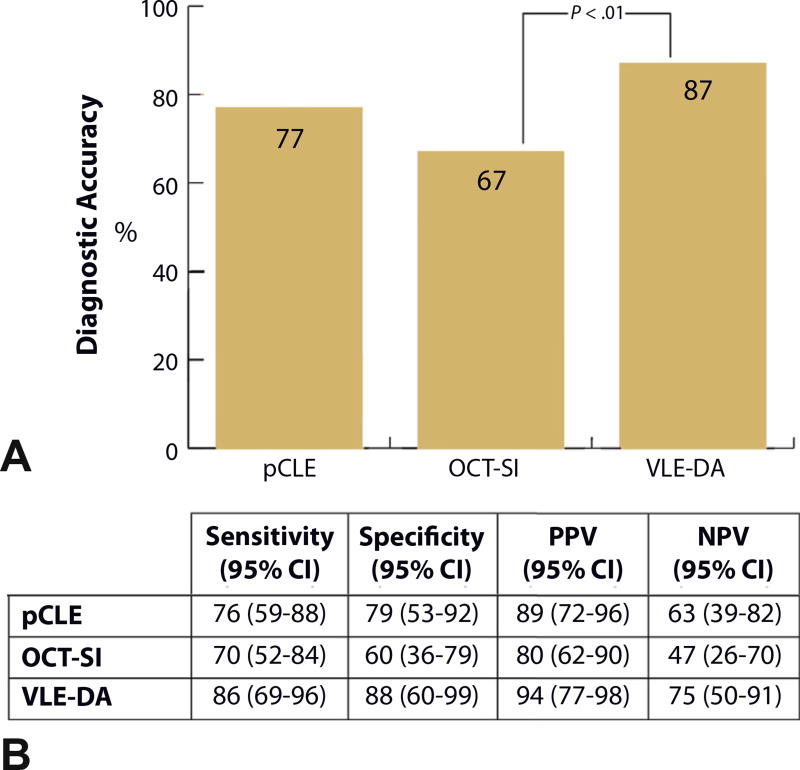
Results: The sensitivity, specificity, and diagnostic accuracy of pCLE for detection of BE dysplasia was 76% (95% confidence interval [CI], 59-88), 79% (95% CI, 53-92), and 77% (95% CI, 72-82), respectively. The optimal diagnostic performance of OCT-SI showed a sensitivity of 70% (95% CI, 52-84), specificity of 60% (95% CI, 36-79), and diagnostic accuracy of 67%; (95% CI, 58-78). The use of the novel VLE-DA showed a sensitivity of 86% (95% CI, 69-96), specificity of 88% (95% CI, 60-99), and diagnostic accuracy of 87% (95% CI, 86-88). The diagnostic accuracy of using the new VLE-DA criteria was significantly superior to the current OCT-SI (P < .01).
Conclusion: The use of a new VLE-DA showed enhanced diagnostic performance for detecting BE dysplasia ex vivo compared with the current OCT-SI. Further validation of this algorithm in vivo is warranted.
Copyright © 2016. Published by Elsevier Inc.
Figures
References
-
- Pohl H, Welch HG. The role of overdiagnosis and reclassification in the marked increase of esophageal adenocarcinoma incidence. J Natl Cancer Inst. 2005;97:142–6. - PubMed
-
- Sharma P, Meining AR, Coron E, et al. Real-time increased detection of neoplastic tissue in Barrett’s esophagus with probe-based confocal laser endomicroscopy: final results of an international multicenter, prospective, randomized, controlled trial. Gastrointest Endosc. 2011;74:465–72. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
