

COLLABORATIVE CARE FOR PERINATAL DEPRESSION IN SOCIOECONOMICALLY DISADVANTAGED WOMEN: A RANDOMIZED TRIAL
- PMID: 26345179
- PMCID: PMC4630126
- DOI: 10.1002/da.22405
COLLABORATIVE CARE FOR PERINATAL DEPRESSION IN SOCIOECONOMICALLY DISADVANTAGED WOMEN: A RANDOMIZED TRIAL
Abstract
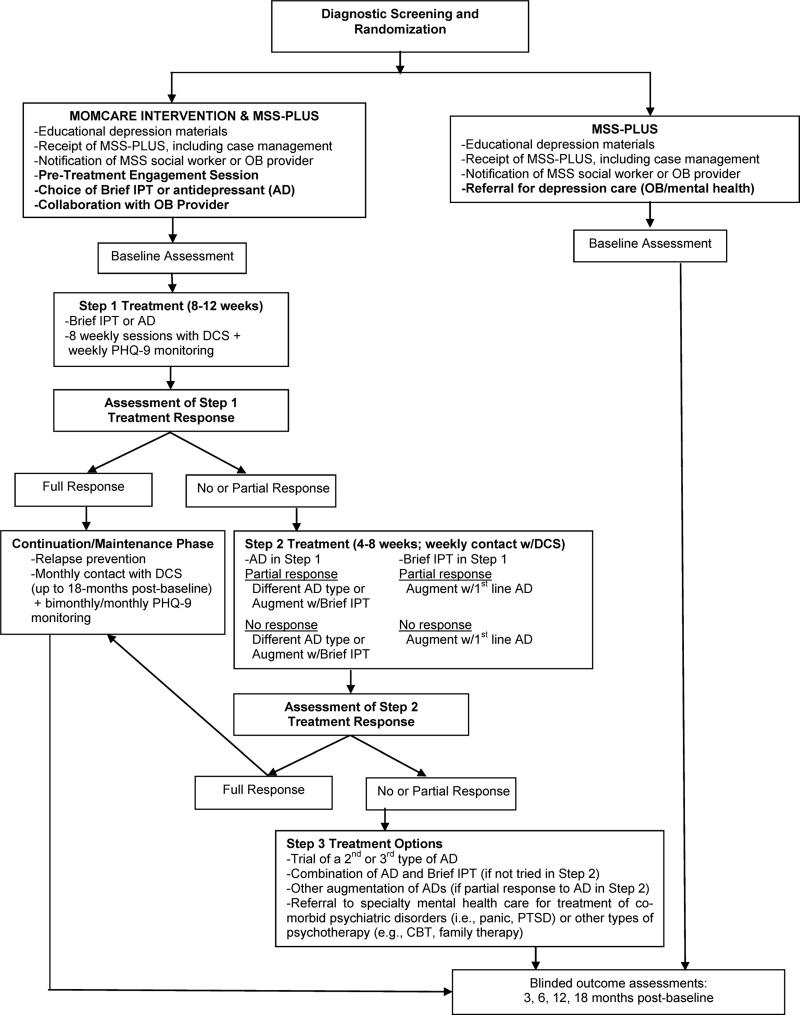
Background: Both antenatal and postpartum depression have adverse, lasting effects on maternal and child well-being. Socioeconomically disadvantaged women are at increased risk for perinatal depression and have experienced difficulty accessing evidence-based depression care. The authors evaluated whether "MOMCare,"a culturally relevant, collaborative care intervention, providing a choice of brief interpersonal psychotherapy and/or antidepressants, is associated with improved quality of care and depressive outcomes compared to intensive public health Maternity Support Services (MSS-Plus).
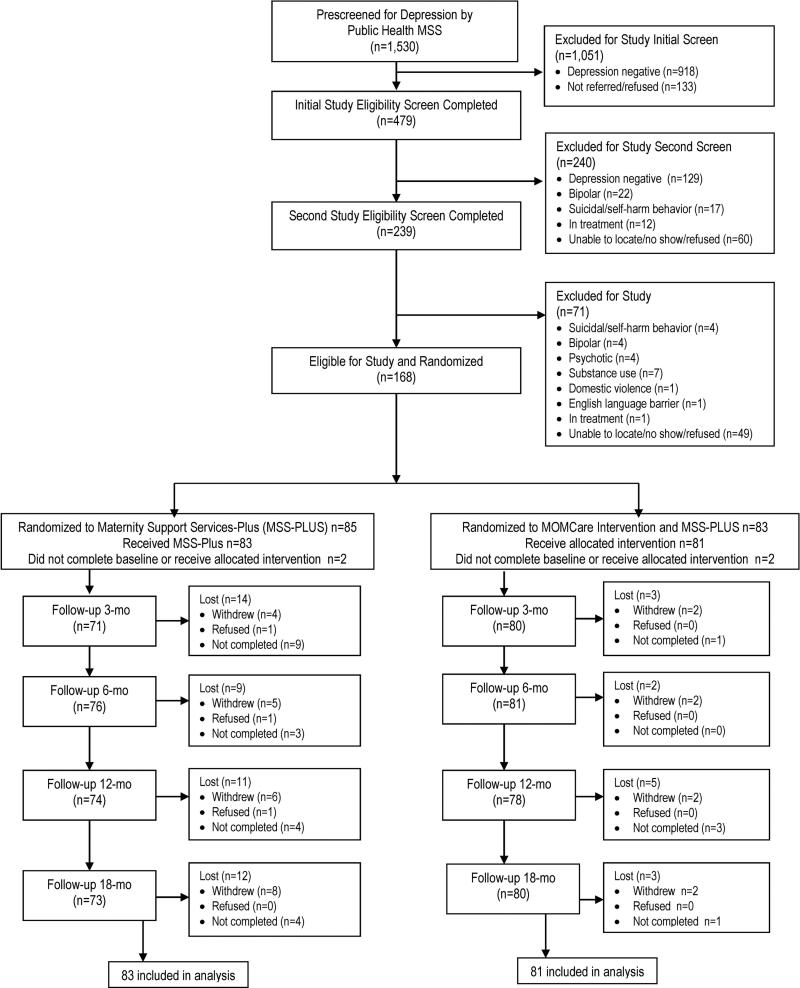
Methods: A randomized multisite controlled trial with blinded outcome assessment was conducted in the Seattle-King County Public Health System. From January 2010 to July 2012, pregnant women were recruited who met criteria for probable major depression and/or dysthymia, English-speaking, had telephone access, and ≥18 years old. The primary outcome was depression severity at 3-, 6-, 12-, 18-month postbaseline assessments; secondary outcomes included functional improvement, PTSD severity, depression response and remission, and quality of depression care.
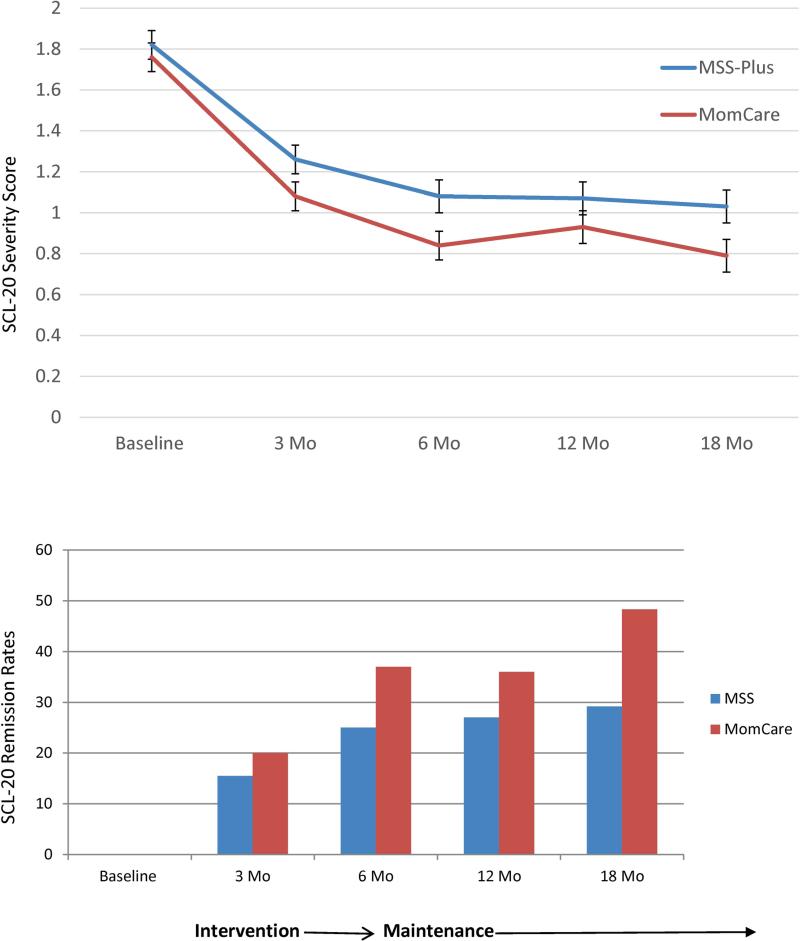
Results: All participants were on Medicaid and 27 years old on average; 58% were non-White; 71% were unmarried; and 65% had probable PTSD. From before birth to 18 months postbaseline, MOMCare (n = 83) compared to MSS-Plus participants (n = 85) attained significantly lower levels of depression severity (Wald's χ(2) = 6.09, df = 1, P = .01) and PTSD severity (Wald's χ(2) = 4.61, df = 1, P = .04), higher rates of depression remission (Wald's χ(2) = 3.67, df = 1, P = .05), and had a greater likelihood of receiving ≥4 mental health visits (Wald's χ(2) = 58.23, df = 1, P < .0001) and of adhering to antidepressants in the prior month (Wald's χ(2) = 10.00, df = 1, P < .01).
Conclusion: Compared to MSS-Plus, MOMCare showed significant improvement in quality of care, depression severity, and remission rates from before birth to 18 months postbaseline for socioeconomically disadvantaged women. Findings suggest that evidence-based perinatal depression care can be integrated into the services of a county public health system in the United States.
Clinical trial registration: ClinicalTrials.govNCT01045655.
Keywords: PTSD; antenatal depression; antidepressants; collaborative care; interpersonal psychotherapy; perinatal depression.
© 2015 Wiley Periodicals, Inc.
Figures
References
-
- O'Hara M, Swain A. Rates and risk of postpartum depression: a meta-analysis. Int Rev Psychiatry. 1996;8:37–54.
-
- Murray L, Cooper P. The role of infant and maternal factors in postpartum depression, mother-infant interactions, and infant outcome. In: Murray L, Cooper P, editors. Postpartum depression and child development. Guilford; New York: 1997. pp. 111–135.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
