

Cost variation in a laparoscopic cholecystectomy and the association with outcomes across a single health system: implications for standardization and improved resource utilization
- PMID: 26345351
- PMCID: PMC4644363
- DOI: 10.1111/hpb.12500
Cost variation in a laparoscopic cholecystectomy and the association with outcomes across a single health system: implications for standardization and improved resource utilization
Abstract
Background: Payers and regulatory bodies are increasingly placing emphasis on cost containment, quality/outcome measurement and transparent reporting. Significant cost variation occurs in many operative procedures without a clear relationship with outcomes. Clear cost-benefit associations will be necessary to justify expenditures in the era of bundled payment structures.
Methods: All laparoscopic cholecystectomies (LCCKs) performed within a single health system over a 1-year period were analysed for operating room (OR) supply cost. The cost was correlated with American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) outcomes.
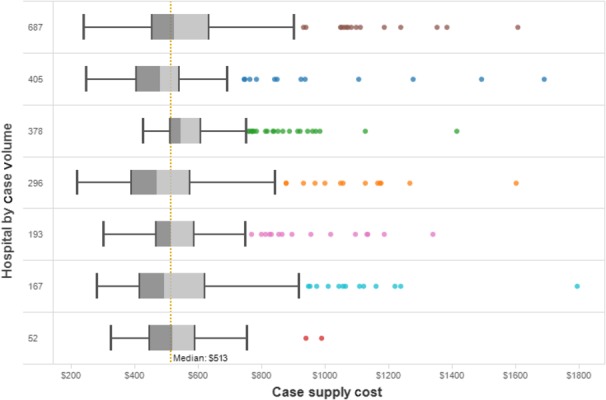
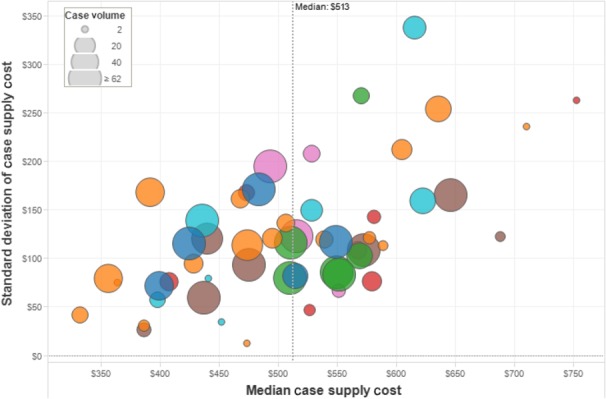
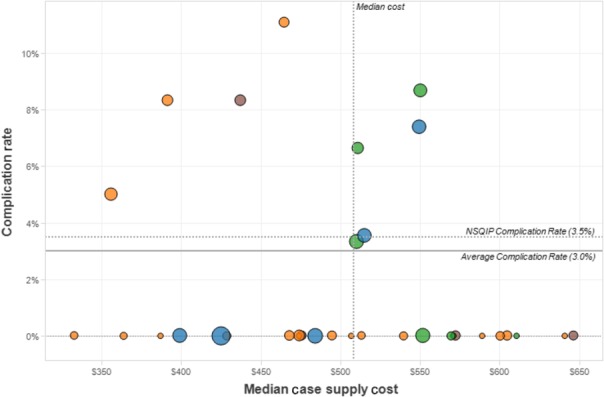
Results: From July 2013 to June 2014, 2178 LCCKs were performed by 55 surgeons at seven hospitals. The median case OR supply cost was $513 ± 156. There was variation in cost between individual surgeons and within an individual surgeon's practice. There was no correlation between cost and ACS NSQIP outcomes. The majority of cost variation was explained by selection of trocar and clip applier constructs.
Conclusions: Significant case OR cost variation is present in LCCK across a single health system, and there is no clear association between increased cost and NSQIP outcomes. Placed within the larger context of overall cost, the opportunity exists for improved resource utilization with no obvious risk for a reduction in the quality of care.
© 2015 International Hepato-Pancreato-Biliary Association.
Figures
References
-
- Center for Medicare and Medicaid. Acute Care Episode Demonstration. Baltimore: . Available at: https://www.cms.gov/Medicare/Demonstration-Projects/DemoProjectsEvalRpts... (last accessed 10 March 2015)
-
- Herman B. 2 major lessons from CMS’ bundled payment ACE demonstration. Becker's Hospital Review. Available at: http://www.beckershospitalreview.com/hospital-physician-relationships/2-... (last accessed 10 March 2015)
-
- Vesely R. An ACE in the deck? Bundled-payment demo shows returns. Mod Healthc. 2011;41:32–33. - PubMed
-
- Casale AS, Paulus RA, Selna MJ, Doll MC, Bothe AE, Jr, McKinley KE, et al. “ProvenCareSM”: a provider-driven pay-for-performance program for acute episodic cardiac surgical care. Ann Surg. 2007;246:613–621. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
