

The Cost Effectiveness of Maintenance Schedules Following Pulmonary Rehabilitation in Patients with Chronic Obstructive Pulmonary Disease: An Economic Evaluation Alongside a Randomised Controlled Trial
- PMID: 26346590
- PMCID: PMC4740569
- DOI: 10.1007/s40258-015-0199-9
The Cost Effectiveness of Maintenance Schedules Following Pulmonary Rehabilitation in Patients with Chronic Obstructive Pulmonary Disease: An Economic Evaluation Alongside a Randomised Controlled Trial
Abstract
Background: Chronic obstructive pulmonary disease (COPD) affects approximately 3 million people in the UK. An 8-week pulmonary rehabilitation (PR) course is recommended under current guidelines. However, studies show that initial benefits diminish over time.
Objective: We present here an economic evaluation conducted alongside a randomised controlled trial (RCT) of a low-intensity maintenance programme over a time horizon of 1 year delivered in UK primary and secondary care settings.
Methods: Patients with COPD who completed at least 60 % of a standard 8-week PR programme were randomised to a 2-h maintenance session at 3, 6 and 9 months (n = 73) or treatment as usual (n = 75). Outcomes were change in Chronic Respiratory Questionnaire (CRQ) score, EQ-5D-based QALYs, cost (price year 2014) to the UK NHS and social services over the 12 months following initial PR, and incremental cost-effectiveness ratios (ICERs).
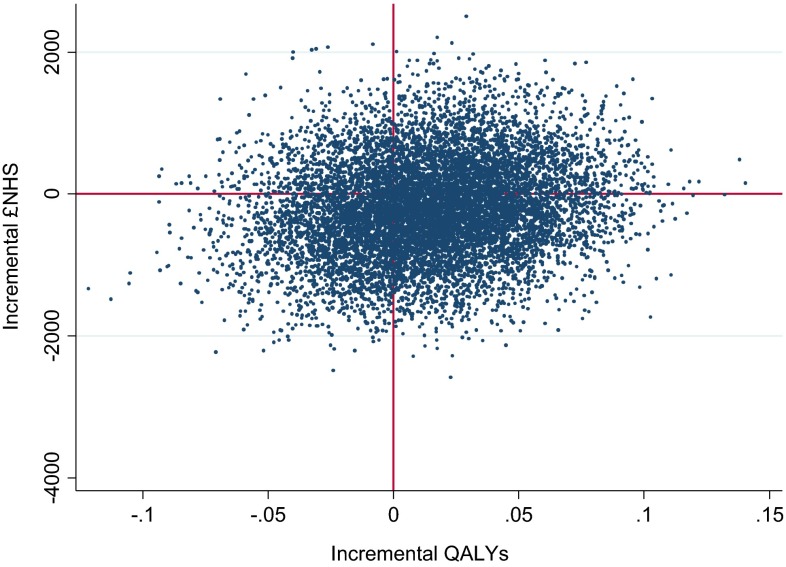
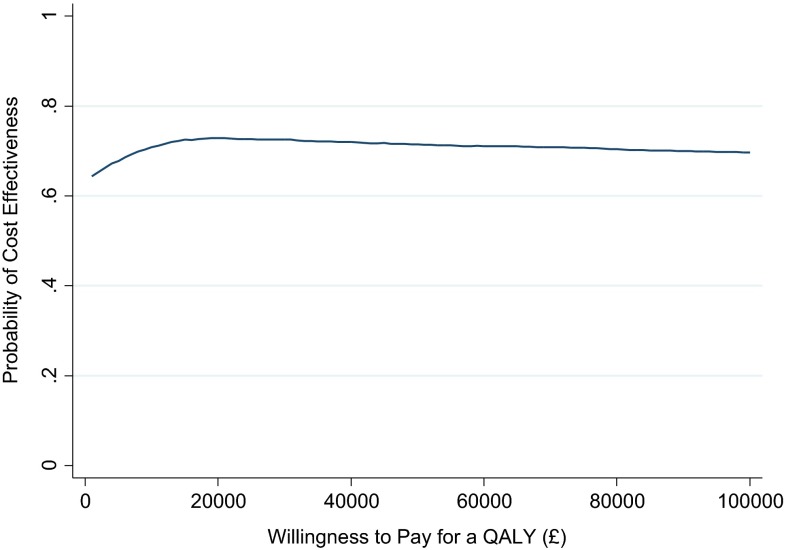
Results: At 12 months, incremental cost to the NHS and social services was -£204.04 (95 % CI -£1522 to £1114). Incremental CRQ and QALY gains were -0.007 (-0.461 to 0.447) and +0.015 (-0.050 to 0.079), respectively. Based on point estimates, PR maintenance therefore dominates treatment as usual from the perspective of the NHS and social services in terms of cost per QALY gained. Whether it is cost effective in terms of CRQ depends on whether the £204 per patient could be reinvested elsewhere to a CRQ gain of greater than 0.007. However, there is much decision uncertainty: 95 % CIs around increments did not exclude zero, and there is a 72.9 % (72.5 %) probability that the ICER is below £20,000 (£30,000) per QALY.
Conclusion: Future research should explore whether more intensive maintenance regimens offer benefit to patients at reasonable cost.
Figures
References
-
- National Institute for Health and Clinical Excellence. Chronic obstructive pulmonary disease. Costing report: implementing NICE guidance. NICE clinical guideline 101. London: National Institute for Health and Clinical Excellence; 2010.
-
- National Institute for Health and Clinical Excellence . Chronic obstructive pulmonary disease: management of chronic obstructive pulmonary disease in adults in primary and secondary care. London: National Institute for Health and Clinical Excellence; 2010.
-
- Bolton CE, Bevan-Smith EF, Blakey JD, et al. British Thoracic Society guideline on pulmonary rehabilitation in adults. Thorax. 2013;68 Suppl 2:ii1–30. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
