

Prognosis Relevance of Serum Cytokines in Pancreatic Cancer
- PMID: 26346854
- PMCID: PMC4539422
- DOI: 10.1155/2015/518284
Prognosis Relevance of Serum Cytokines in Pancreatic Cancer
Abstract
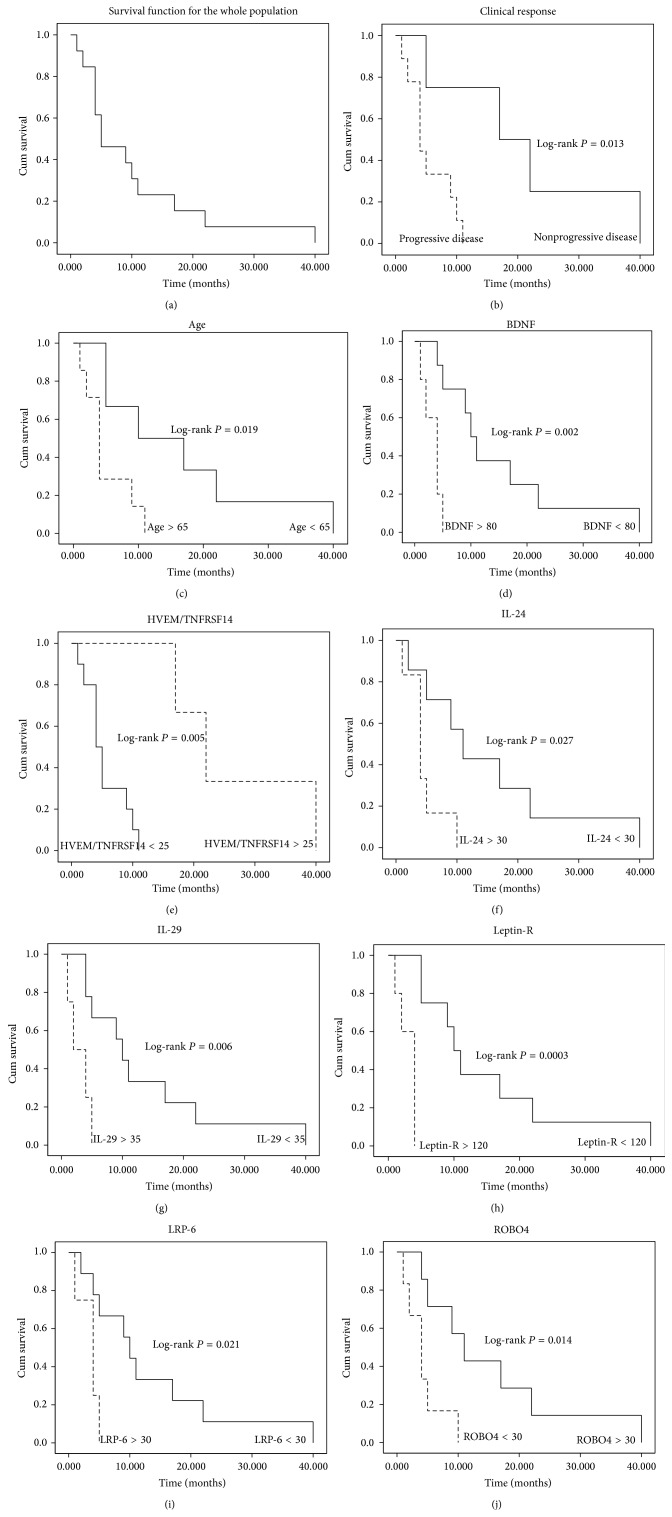
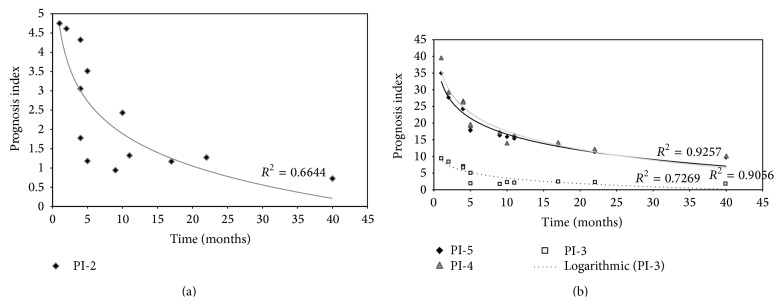
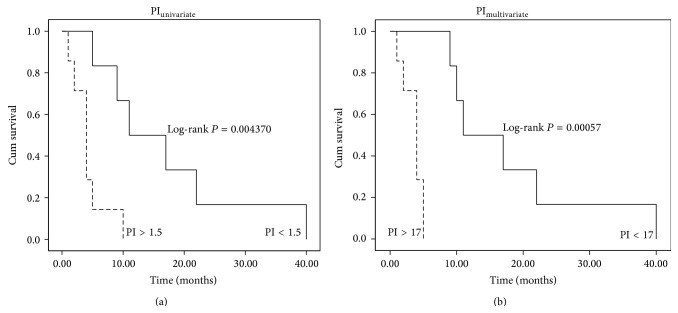
The overall survival of patients with pancreatic ductal adenocarcinoma is extremely low. Although gemcitabine is the standard used chemotherapy for this disease, clinical outcomes do not reflect significant improvements, not even when combined with adjuvant treatments. There is an urgent need for prognosis markers to be found. The aim of this study was to analyze the potential value of serum cytokines to find a profile that can predict the clinical outcome in patients with pancreatic cancer and to establish a practical prognosis index that significantly predicts patients' outcomes. We have conducted an extensive analysis of serum prognosis biomarkers using an antibody array comprising 507 human cytokines. Overall survival was estimated using the Kaplan-Meier method. Univariate and multivariate Cox's proportional hazard models were used to analyze prognosis factors. To determine the extent that survival could be predicted based on this index, we used the leave-one-out cross-validation model. The multivariate model showed a better performance and it could represent a novel panel of serum cytokines that correlates to poor prognosis in pancreatic cancer. B7-1/CD80, EG-VEGF/PK1, IL-29, NRG1-beta1/HRG1-beta1, and PD-ECGF expressions portend a poor prognosis for patients with pancreatic cancer and these cytokines could represent novel therapeutic targets for this disease.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
