

Feasibility and Safety of Using External Counterpulsation to Augment Cerebral Blood Flow in Acute Ischemic Stroke-The Counterpulsation to Upgrade Forward Flow in Stroke (CUFFS) Trial
- PMID: 26347398
- PMCID: PMC4630102
- DOI: 10.1016/j.jstrokecerebrovasdis.2015.07.013
Feasibility and Safety of Using External Counterpulsation to Augment Cerebral Blood Flow in Acute Ischemic Stroke-The Counterpulsation to Upgrade Forward Flow in Stroke (CUFFS) Trial
Abstract
Background: External counterpulsation (ECP) increases perfusion to a variety of organs and may be helpful for acute stroke.
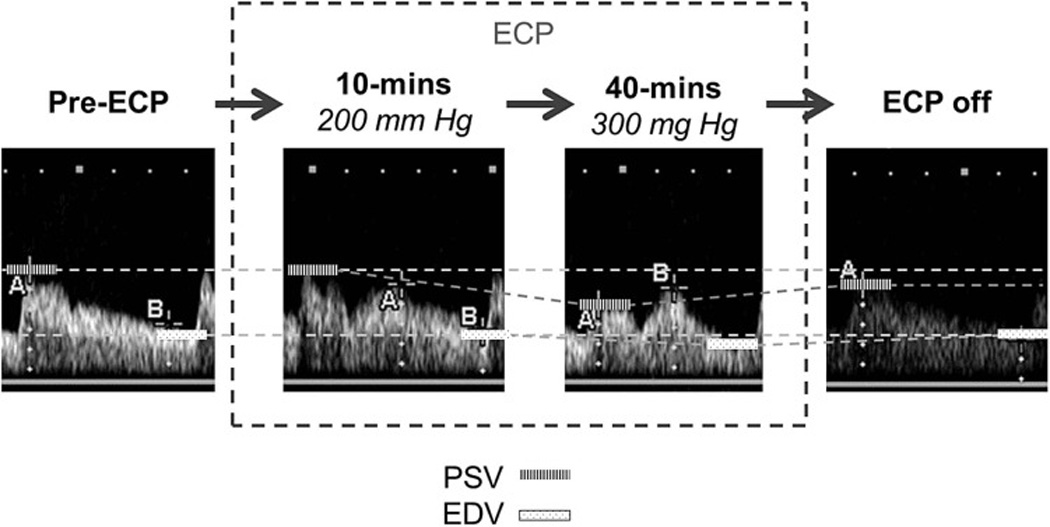
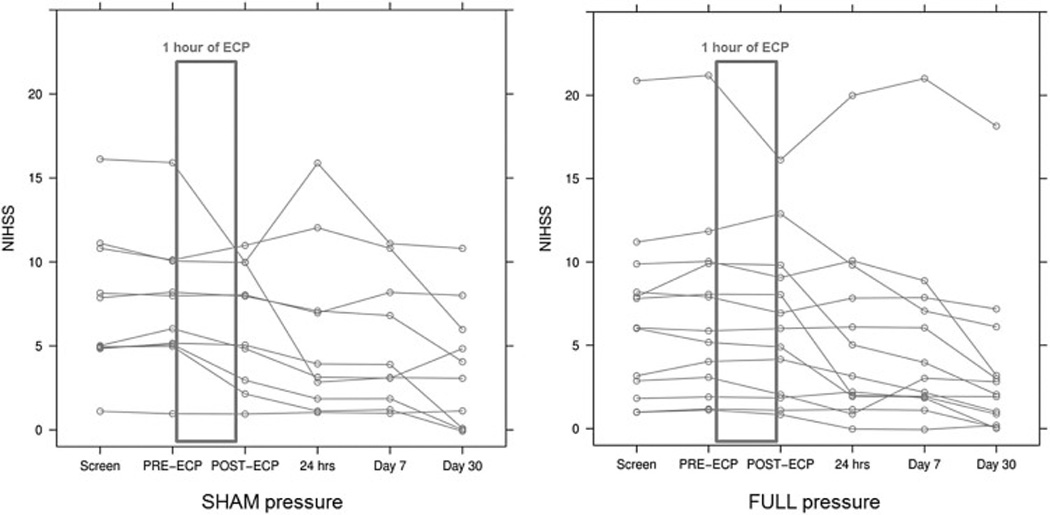
Methods: We conducted a single-blinded, prospective, randomized controlled feasibility and safety trial of ECP for acute middle cerebral artery (MCA) ischemic stroke. Twenty-three patients presenting within 48 hours of symptom onset were randomized into one of two groups. One group was treated with ECP for 1 hour at a pressure of up to 300 mmHg ("full pressure"). During the procedure, we also determined the highest possible pressure that would augment MCA mean flow velocity (MFV) by 15%. The other group was treated with ECP at 75 mmHg ("sham pressure"). Transcranial Doppler MCA flow velocities and National Institutes of Health Stroke Scale (NIHSS) scores of both groups were checked before, during, and after ECP. Outcomes were assessed at 30 days after randomization.
Results: Although the procedures were feasible to implement, there was a frequent inability to augment MFV by 15% despite maximal pressures in full-pressure patients. In sham-pressure patients, however, MFV frequently increased as shown by increases in peak systolic velocity and end diastolic velocity. In both groups, starting ECP was often associated with contemporaneous improvements in NIHSS stroke scores. There were no between-group differences in NIHSS, modified Rankin Scale Scores, and Barthel Indices, and no device or treatment-related serious adverse events, deaths, intracerebral hemorrhages, or episodes of acute neuro-worsening.
Conclusions: ECP was safe and feasible to use in patients with acute ischemic stroke. It was associated with unexpected effects on flow velocity, and contemporaneous improvements in NIHSS score regardless of pressure used, with a possibility that even very low ECP pressures had an effect. Further study is warranted.
Keywords: Cerebral blood flow velocity; External counterpulsation; Ischemic stroke; Transcranial Doppler.
Copyright © 2015 National Stroke Association. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Applebaum RM, Kasliwal R, Tunick PA, et al. Sequential external counterpulsation increases cerebral and renal blood flow. Am Heart J. 1997;133:611–615. - PubMed
-
- Werner D, Schneider M, Weise M, Nonnast-Daniel B, Daniel WG. Pneumatic external counterpulsation: a new noninvasive method to improve organ perfusion. Am J Cardiol. 1999;84:950–952. - PubMed
-
- Hilz MJ, Werner D, Marthol H, Flachskampf FA, Daniel WG. Enhanced external counterpulsation improves skin oxygenation and perfusion. Eur J Clin Invest. 2004;34(6):385–391. - PubMed
-
- Werner D, Tragner P, Wawer A, Porst H, Daniel WG, Gross P. Enhanced external counterpulsation: a new technique to augment renal function in liver cirrhosis. Nephrol Dial Transplant. 2005;20(5):920–926. - PubMed
-
- Arora RR, Chou TM, Jain D, Fleishman B, Crawford L, McKiernan T, Nesto RW. The multicenter study of enhanced external counterpulsation (MUST-EECP): effect of EECP on exercise-induced myocardial ischemia and angina episodes. J Am Coll Cardiol. 1999;33:1833–1840. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
