

A Prospective Pilot Trial for Pallidal Deep Brain Stimulation in Huntington's Disease
- PMID: 26347707
- PMCID: PMC4539552
- DOI: 10.3389/fneur.2015.00177
A Prospective Pilot Trial for Pallidal Deep Brain Stimulation in Huntington's Disease
Abstract
Background: Movement disorders in Huntington's disease are often medically refractive. The aim of the trial was assessment of procedure safety of deep brain stimulation, equality of internal- and external-pallidal stimulation and efficacy followed-up for 6 months in a prospective pilot trial.
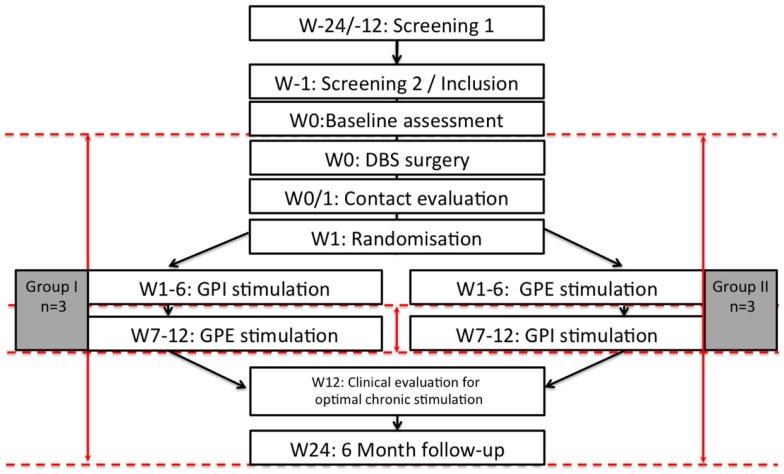
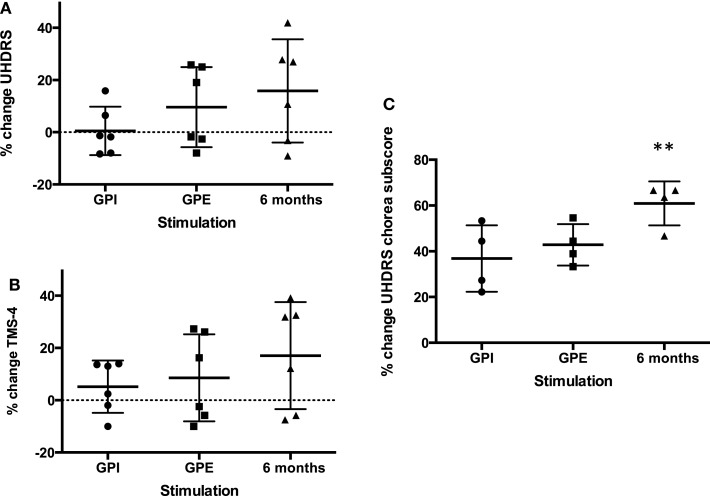
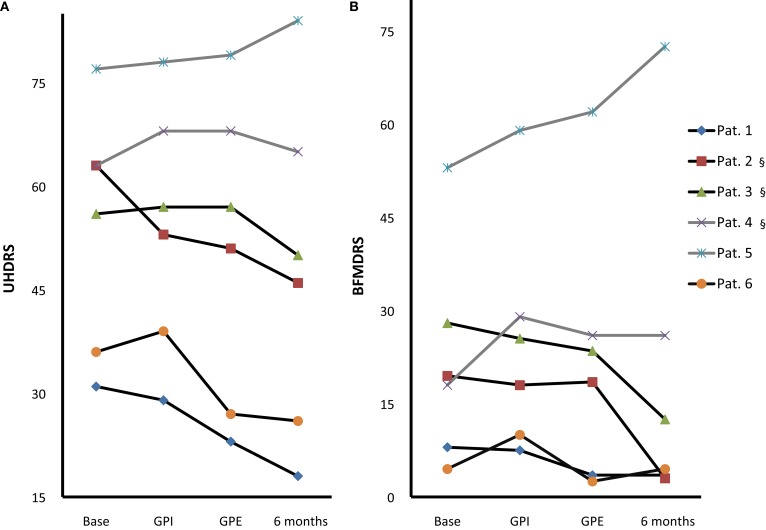
Methods: In a controlled double-blind phase six patients (four chorea-dominant, two Westphal-variant) with predominant movement disorder were randomly assigned to either the sequence of 6-week internal- or 6-week external-pallidal stimulation, or vice versa, followed by further 3 months chronic pallidal stimulation at the target with best effect-side-effect ratio. Primary endpoints were changes in the Unified Huntington's Disease Rating Scale motor-score, chorea subscore, and total motor-score 4 (blinded-video ratings), comparing internal- versus external-pallidal stimulation, and 6 months versus baseline. Secondary endpoints assessed scores on dystonia, hypokinesia, cognition, mood, functionality/disability, and quality-of-life.
Results: Intention-to-treat analysis of all patients (n = 3 in each treatment sequence): Both targets were equal in terms of efficacy. Chorea subscores decreased significantly over 6 months (-5.3 (60.2%), p = 0.037). Effects on dystonia were not significant over the group due to it consisting of three responders (>50% improvement) and three non-responders. Westphal patients did not improve. Cognition was stable. Mood and some functionality/disability and quality-of-life scores improved significantly. Eight adverse events and two additional serious adverse events - mostly internal-pallidal stimulation-related - resolved without sequalae. No procedure-related complications occurred.
Conclusion: Pallidal deep brain stimulation was demonstrated to be a safe treatment option for the reduction of chorea in Huntington's disease. Their effects on chorea and dystonia and on quality-of-life should be examined in larger controlled trials.
Keywords: chorea; deep brain stimulation; pallidum; Huntington's Disease.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical