

The Diagnostic and Therapeutic Challenges of Posttraumatic Iris Implantation Cysts: Illustrative Case Presentations and a Review of the Literature
- PMID: 26347837
- PMCID: PMC4549539
- DOI: 10.1155/2015/375947
The Diagnostic and Therapeutic Challenges of Posttraumatic Iris Implantation Cysts: Illustrative Case Presentations and a Review of the Literature
Abstract
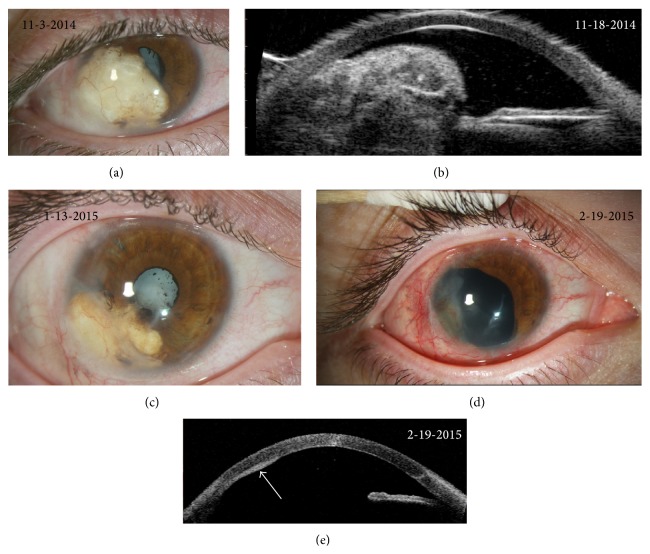
Posttraumatic iris implantation cysts are rare ocular findings that are often associated with poor visual outcomes. Iris implantation cysts can present clinicians with diagnostic and therapeutic challenges given their variable presentations and frequently destructive nature. In this paper, we provide descriptions of two unusual cases of posttraumatic iris implantation cysts. The first case is of a recurrent keratin-filled iris implantation cyst that developed after open globe injury and intraocular implantation of cilia and was treated with cyst debulking procedures, injections of 5-Fluorouracil, and iridocyclectomy. The second case is of recurrent posttraumatic serous iris implantation cysts that were treated with laser, cyst aspiration, and injections of 5-Fluorouracil. We use these cases as a platform to discuss the different manifestations of implantation cysts, the roles of anterior segment optical coherence tomography, ultrasound biomicroscopy, and histopathology in facilitating timely and accurate diagnosis and review the range of available therapeutic modalities. We discuss conservative treatment approaches, including the novel use of 5-Fluorouracil therapy as an adjunct therapy, as well as more aggressive surgical excision requiring ocular reconstruction. Through a discussion of these cases and review of the literature, we provide recommendations to assist clinicians in managing this uncommon but vision-threatening condition and minimizing complications.
Figures




Similar articles
-
Implantation iris cysts developing 24 years after penetrating keratoplasty.Am J Ophthalmol Case Rep. 2022 Jan 31;25:101340. doi: 10.1016/j.ajoc.2022.101340. eCollection 2022 Mar. Am J Ophthalmol Case Rep. 2022. PMID: 35146204 Free PMC article.
-
Iris Cyst.2024 Feb 28. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2024 Feb 28. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 34662087 Free Books & Documents.
-
Iris cyst after iris-sutured intraocular lens implantation in a child.J AAPOS. 2012 Apr;16(2):199-200. doi: 10.1016/j.jaapos.2011.12.147. J AAPOS. 2012. PMID: 22525181
-
Cysts and tumours of the iris: Diagnostic tools and key management considerations-A review.Clin Exp Ophthalmol. 2024 Aug;52(6):665-683. doi: 10.1111/ceo.14380. Epub 2024 Apr 5. Clin Exp Ophthalmol. 2024. PMID: 38577954 Review.
-
Iris cysts: A comprehensive review on diagnosis and treatment.Surv Ophthalmol. 2018 May-Jun;63(3):347-364. doi: 10.1016/j.survophthal.2017.08.009. Epub 2017 Sep 5. Surv Ophthalmol. 2018. PMID: 28882598 Review.
Cited by
-
Iris implantation cysts growth five decades after trauma.Am J Ophthalmol Case Rep. 2025 Apr 11;38:102333. doi: 10.1016/j.ajoc.2025.102333. eCollection 2025 Jun. Am J Ophthalmol Case Rep. 2025. PMID: 40297822 Free PMC article.
-
[Cyst of the anterior chamber after uneventful cataract surgery].Ophthalmologie. 2022 Aug;119(8):845-847. doi: 10.1007/s00347-021-01463-9. Epub 2021 Aug 2. Ophthalmologie. 2022. PMID: 34338848 German. No abstract available.
-
Sterile iris abscess associated with herpes zoster ophthalmicus.Am J Ophthalmol Case Rep. 2021 Jun 17;23:101144. doi: 10.1016/j.ajoc.2021.101144. eCollection 2021 Sep. Am J Ophthalmol Case Rep. 2021. PMID: 34195477 Free PMC article.
References
-
- Rizzuti A. B. Traumatic implantation cysts of the iris; with special emphasis on surgical aspects. American Journal of Ophthalmology. 1955;39(1):13–20. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
