

Management of Menopausal Symptoms
- PMID: 26348174
- PMCID: PMC4594172
- DOI: 10.1097/AOG.0000000000001058
Management of Menopausal Symptoms
Abstract
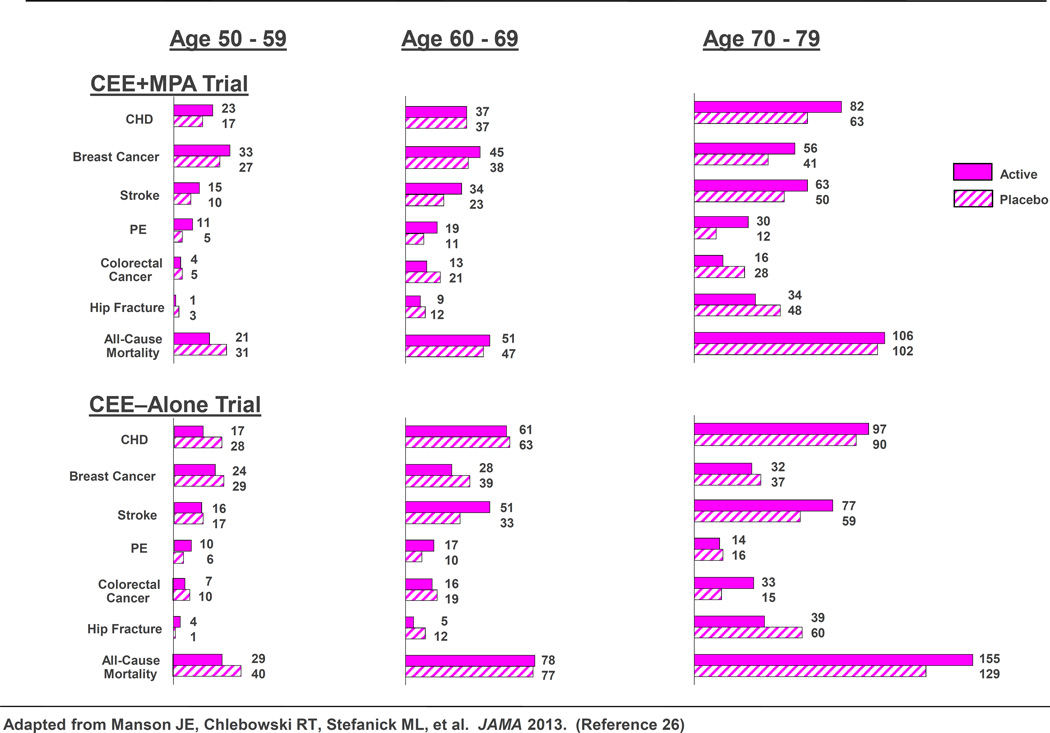
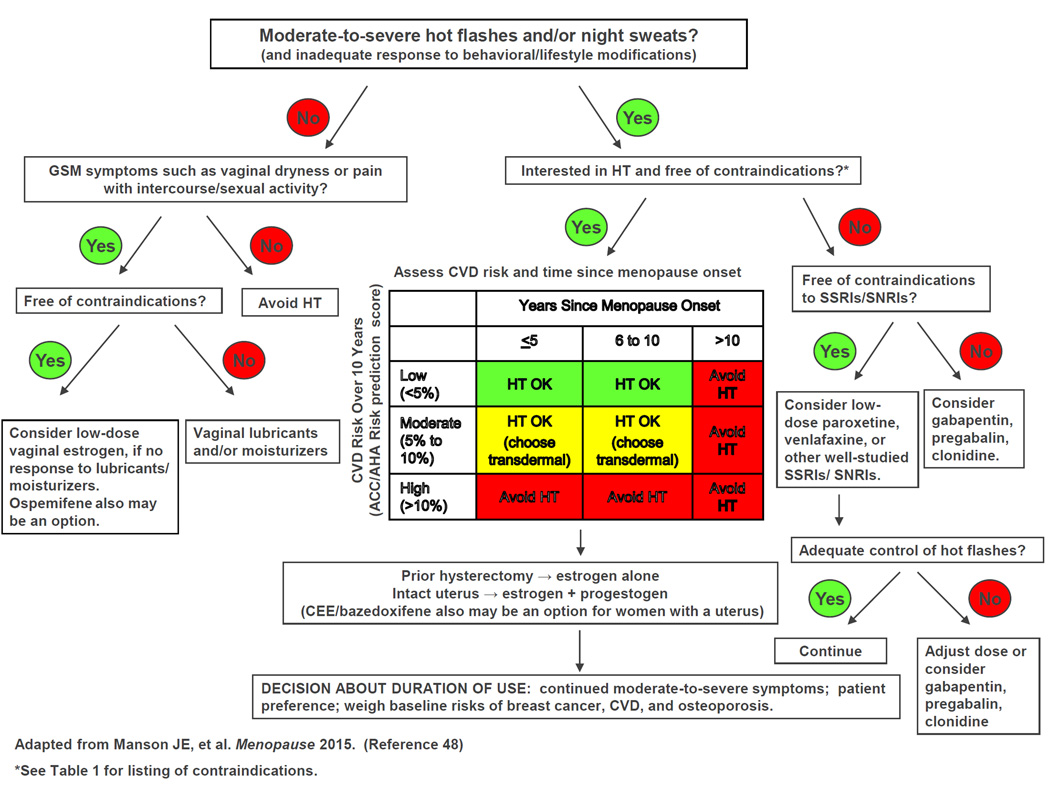
Most menopausal women experience vasomotor symptoms with bothersome symptoms often lasting longer than one decade. Hormone therapy (HT) represents the most effective treatment for these symptoms with oral and transdermal estrogen formulations having comparable efficacy. Findings from the Women's Health Initiative and other recent randomized clinical trials have helped to clarify the benefits and risks of combination estrogen-progestin and estrogen-alone therapy. Absolute risks observed with HT tended to be small, especially in younger women. Neither regimen increased all-cause mortality rates. Given the lower rates of adverse events on HT among women close to menopause onset and at lower baseline risk of cardiovascular disease, risk stratification and personalized risk assessment appear to represent a sound strategy for optimizing the benefit-risk profile and safety of HT. Systemic HT should not be arbitrarily stopped at age 65 years; instead treatment duration should be individualized based on patients' risk profiles and personal preferences. Genitourinary syndrome of menopause represents a common condition that adversely affects the quality of life of many menopausal women. Without treatment, symptoms worsen over time. Low-dose vaginal estrogen represents highly effective treatment for this condition. Because custom-compounded hormones have not been tested for efficacy or safety, U.S. Food and Drug Administration (FDA)-approved HT is preferred. A low-dose formulation of paroxetine mesylate currently represents the only nonhormonal medication FDA-approved to treat vasomotor symptoms. Gynecologists and other clinicians who remain abreast of data addressing the benefit-risk profile of hormonal and nonhormonal treatments can help menopausal women make sound choices regarding management of menopausal symptoms.
Conflict of interest statement
Financial Disclosure:
Dr. Manson did not report any potential conflicts of interest.
Figures
References
-
- North American Menopause Society, Menopause Practice: A Clinician's Guide. 5th Ed. 2014.
-
- Nelson HD. Menopause (Seminar) Lancet. 2008;371:760–770. - PubMed
-
- Freedman RR. Physiology of hot flashes. American journal of human biology : the official journal of the Human Biology Council. 2001;13:453–464. - PubMed
-
- Casper RF, Yen SS. Neuroendocrinology of menopausal flushes: an hypothesis of flush mechanism. Clinical endocrinology. 1985;22:293–312. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
