

The Association of Expanded Access to a Collaborative Midwifery and Laborist Model With Cesarean Delivery Rates
- PMID: 26348175
- PMCID: PMC4580519
- DOI: 10.1097/AOG.0000000000001032
The Association of Expanded Access to a Collaborative Midwifery and Laborist Model With Cesarean Delivery Rates
Abstract
Objective: To examine the association between expanded access to collaborative midwifery and laborist services and cesarean delivery rates.
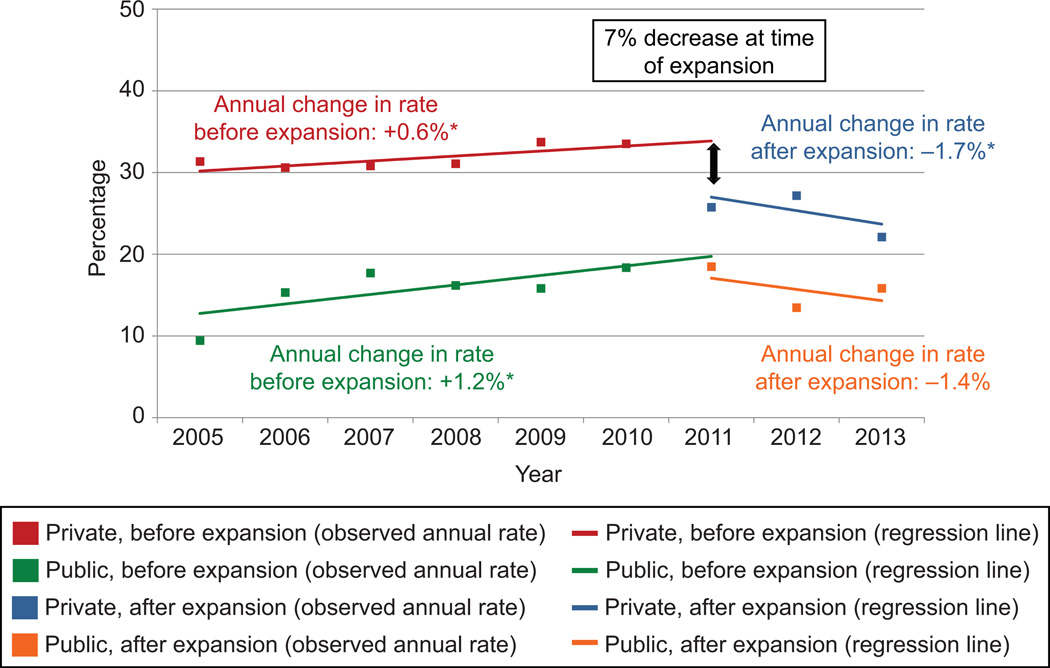
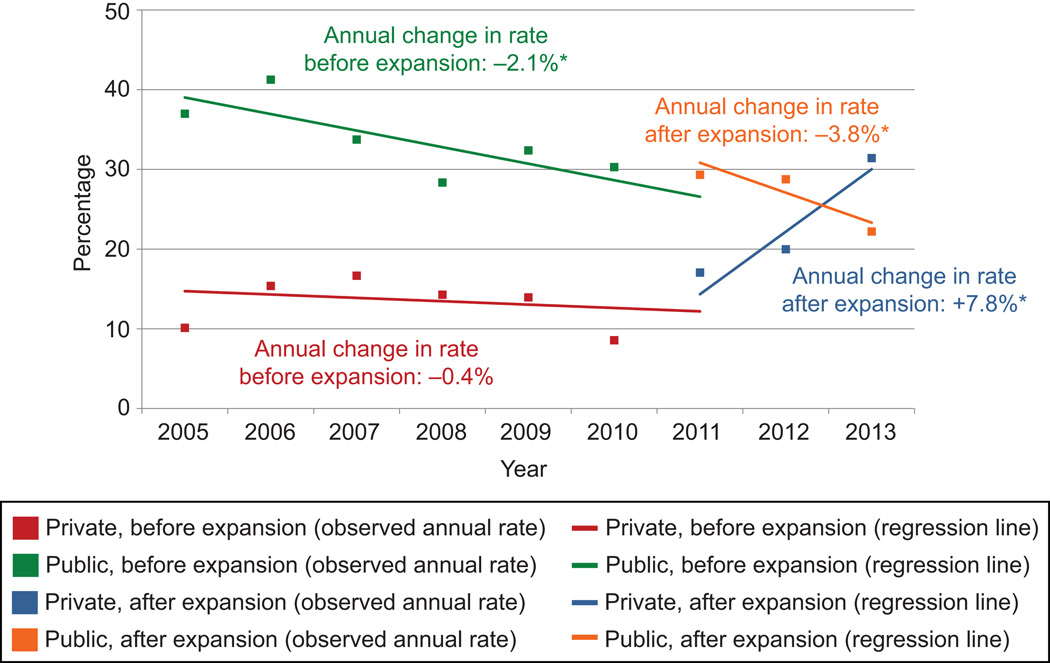
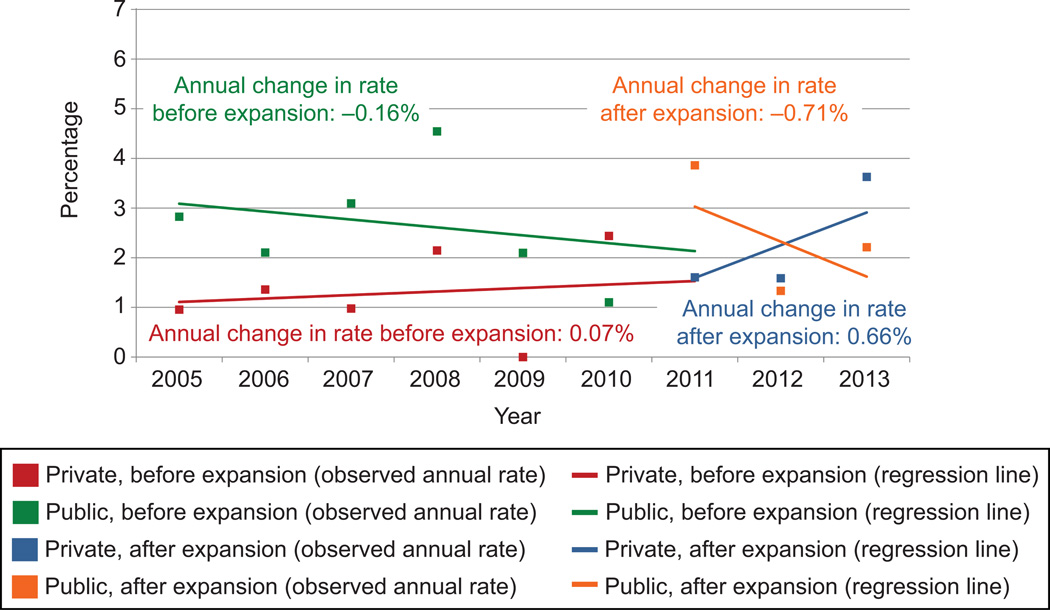
Methods: This was a prospective cohort study at a community hospital between 2005 and 2014. In 2011, privately insured women changed from a private practice model to one that included 24-hour midwifery and laborist coverage. Primary cesarean delivery rates among nulliparous, term, singleton, vertex women and vaginal birth after cesarean delivery (VBAC) rates among women with prior cesarean delivery were compared before and after the change. Multivariable logistic regression models estimated the effects of the change on the odds of primary cesarean delivery and VBAC; an interrupted time-series analysis estimated the annual rates before and after the expansion.
Results: There were 3,560 nulliparous term singleton vertex deliveries and 1,324 deliveries with prior cesarean delivery during the study period; 45% were among privately insured women whose care model changed. The primary cesarean delivery rate among these privately insured women decreased after the change, from 31.7% to 25.0% (P=.005, adjusted odds ratio [OR] 0.56, 95% confidence interval [CI] 0.39-0.81). The interrupted time-series analysis estimated a 7% drop in the primary cesarean delivery rate in the year after the expansion and a decrease of 1.7% per year thereafter. The VBAC rate increased from 13.3% before to 22.4% afterward (adjusted OR 2.03, 95% CI 1.08-3.80).
Conclusion: The change from a private practice to a collaborative midwifery-laborist model was associated with a decrease in primary cesarean rates and an increase in VBAC rates.
Level of evidence: II.
Conflict of interest statement
Figures
References
-
- Podulka J, Stranges E, Steiner C. Hospitalizations Related to Childbirth, 2008. Rockville, MD: Agency for Healthcare Research and Quality; 2011. Apr, [cited February 18, 2013]. HCUP Statistical Brief #110. HCUP Statistical Brief #110. ed. - PubMed
-
- March of Dimes Peristats. March of Dimes. [cited May 31, 2013];2013 [Internet] Available from: www.marchofdimes.com/peristats.
-
- Callaghan WM, Creanga AA, Kuklina EV. Severe maternal morbidity among delivery and postpartum hospitalizations in the United States. Obstet Gynecol. 2012 Nov;120(5):1029–1036. - PubMed
-
- Clark SL, Belfort MA, Dildy GA, Meyers JA. Reducing obstetric litigation through alterations in practice patterns. Obstet Gynecol. 2008 Dec;112(6):1279–1283. - PubMed
-
- Olson R, Garite TJ, Fishman A, Andress IF. Obstetrician/gynecologist hospitalists: can we improve safety and outcomes for patients and hospitals and improve lifestyle for physicians? Am J Obstet Gynecol. 2012 Aug;207(2):81–86. - PubMed
