

The Addition of Postoperative Chemotherapy is Associated with Improved Survival in Patients with Pancreatic Cancer Treated with Preoperative Therapy
- PMID: 26350371
- PMCID: PMC5192562
- DOI: 10.1245/s10434-015-4854-z
The Addition of Postoperative Chemotherapy is Associated with Improved Survival in Patients with Pancreatic Cancer Treated with Preoperative Therapy
Abstract
Background: Preoperative/neoadjuvant therapy (NT) is increasingly utilized for the treatment of pancreatic ductal adenocarcinoma (PDAC). However, little data exist regarding information on the use of additional postoperative therapy following NT. The lymph node ratio (LNR) is a prognostic marker of oncologic outcomes after NT and resection. In this study, we evaluated the effectiveness of postoperative therapy following NT, stratified by LNR.
Methods: A prospective tumor registry database was queried to identify patients with PDAC who underwent resection following NT from 1990 to 2008. Clinicopathologic factors were compared to identify associations with overall survival (OS) and time to recurrence (TTR) based on postoperative chemotherapy status.
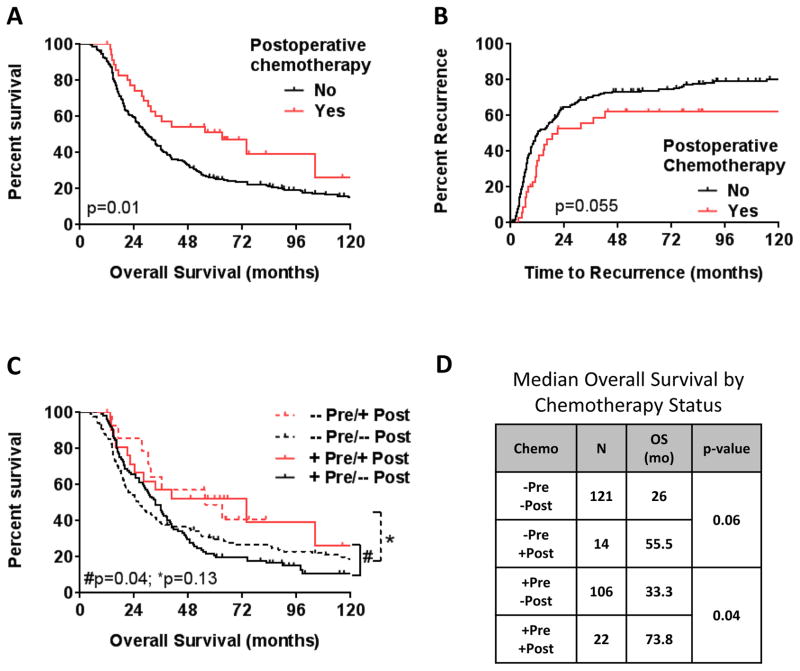
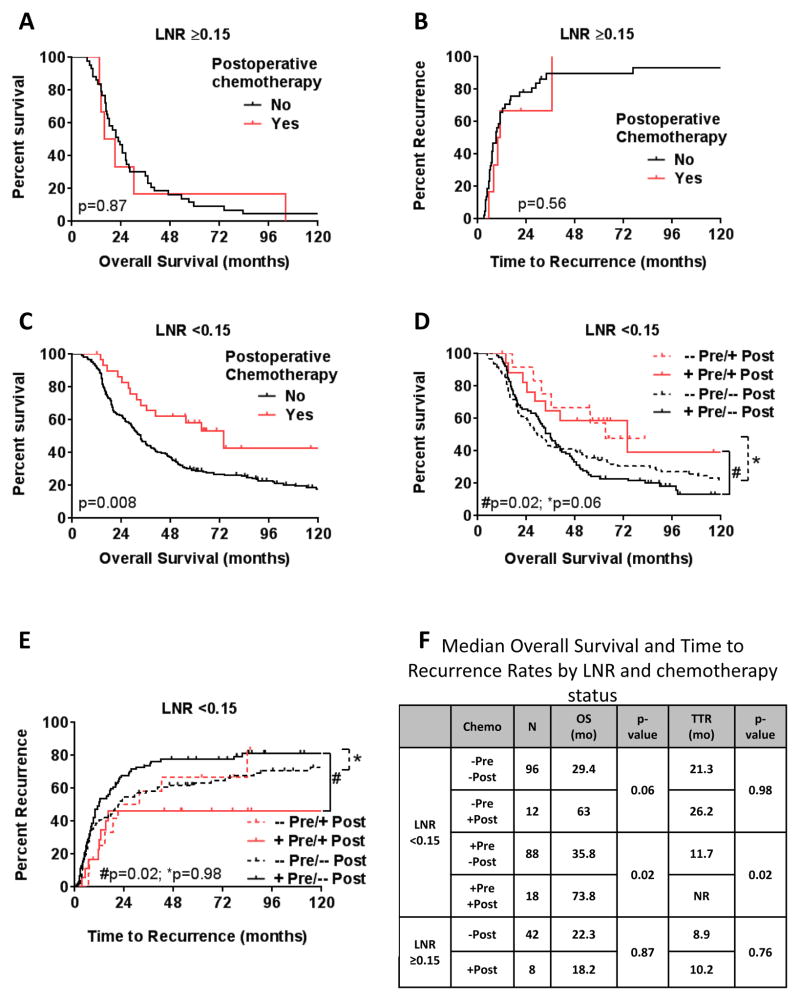
Results: Thirty-six (14 %) of the 263 patients received additional postoperative therapy. No differences were observed in the pathologic characteristics between patients who received postoperative chemotherapy and those who did not. The median LNR was 0.12 for patients with N + disease. Following NT, the administration of postoperative therapy was associated with improved median OS (72 vs. 33 months; p = 0.008) for patients with an LNR < 0.15. There was no association between postoperative chemotherapy and OS for patients with LNR ≥ 0.15. Multivariate analysis demonstrated that the administration of postoperative systemic therapy in patients with a low LNR was associated with a reduced risk of death (hazard ratio 0.49; p = 0.02).
Conclusion: Postoperative chemotherapy after NT in patients with low LNR is associated with improved oncologic outcomes.
Figures
References
-
- Tzeng CW, Tran Cao HS, Lee JE, et al. Treatment sequencing for resectable pancreatic cancer: influence of early metastases and surgical complications on multimodality therapy completion and survival. Journal of gastrointestinal surgery : official journal of the Society for Surgery of the Alimentary Tract. 2014 Jan;18(1):16–24. discussion 24–15. - PubMed
-
- Bilimoria KY, Bentrem DJ, Ko CY, et al. Multimodality therapy for pancreatic cancer in the U.S. : utilization, outcomes, and the effect of hospital volume. Cancer. 2007 Sep 15;110(6):1227–1234. - PubMed
-
- Varadhachary GR, Wolff RA, Crane CH, et al. Preoperative gemcitabine and cisplatin followed by gemcitabine-based chemoradiation for resectable adenocarcinoma of the pancreatic head. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2008 Jul 20;26(21):3487–3495. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
