

Different Somatic Mutations in Multinodular Adrenals With Aldosterone-Producing Adenoma
- PMID: 26351028
- PMCID: PMC4600038
- DOI: 10.1161/HYPERTENSIONAHA.115.05993
Different Somatic Mutations in Multinodular Adrenals With Aldosterone-Producing Adenoma
Abstract
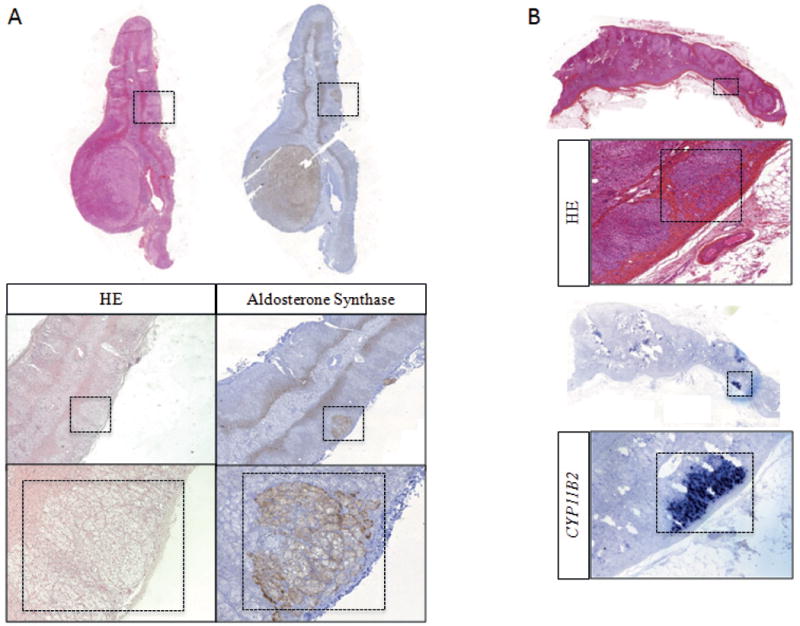
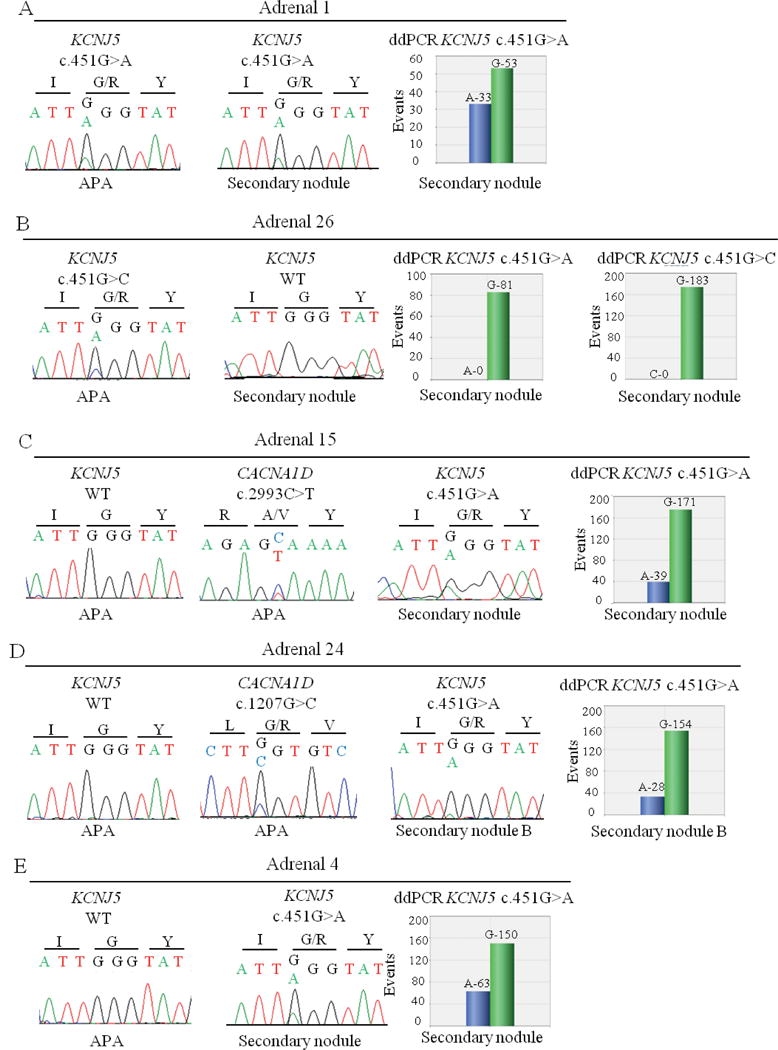
Primary aldosteronism is the most common form of secondary hypertension. Somatic mutations in KCNJ5, ATP1A1, ATP2B3, and CACNA1D are found in aldosterone-producing adenoma. In addition, adrenals with aldosterone-producing adenomas show cortical remodeling and frequently multiple secondary nodules. Our aim was to investigate whether different aldosterone-producing nodules from the same adrenal share the same mutational status. Aldosterone synthase expression was assessed in multinodular adrenals from 27 patients. DNA of 37 aldosterone-producing secondary nodules was extracted from formalin-fixed paraffin-embedded tissues and genotyped for KCNJ5, ATP1A1, ATP2B3, and CACNA1D mutations. Among 17 adrenals with a somatic mutation in the principal nodule, 4 showed the same mutation in a secondary nodule, whereas 10 had no mutation in any of the known genes. In 1 adrenal harboring the KCNJ5 p.Gly151Arg mutation in the principal nodule, the same mutation was present in 2 secondary nodules, but no mutation was found in a third nodule. Finally, in 2 adrenals with a CACNA1D mutation in the principal nodule, a KCNJ5 mutation was identified in the secondary nodule. Among 10 adrenals without mutations in the principal nodule, 1 carried a KCNJ5 mutation in the secondary nodule. No mutations were detected in 7 aldosterone-producing cell clusters from 6 adrenals. No association was observed between the presence of mutations in secondary nodules and clinical parameters. In conclusion, different mutations are found in different aldosterone-producing nodules from the same adrenal, suggesting that somatic mutations are independent events triggered by mechanisms that remain to be identified.
Keywords: adrenal cortex; aldosterone; hyperaldosteronism; mineralocorticoids; mutation; potassium channels.
© 2015 American Heart Association, Inc.
Conflict of interest statement
Figures
References
-
- Rossi GP, Bernini G, Caliumi C, et al. A prospective study of the prevalence of primary aldosteronism in 1,125 hypertensive patients. J Am Coll Cardiol. 2006;48:2293–2300. - PubMed
-
- Hannemann A, Bidlingmaier M, Friedrich N, et al. Screening for primary aldosteronism in hypertensive subjects: results from two German epidemiological studies. Eur J Endocrinol. 2012;167:7–15. - PubMed
-
- Mulatero P, Stowasser M, Loh KC, Fardella CE, Gordon RD, Mosso L, Gomez-Sanchez CE, Veglio F, Young WF., Jr Increased diagnosis of primary aldosteronism, including surgically correctable forms, in centers from five continents. J Clin Endocrinol Metab. 2004;89:1045–1050. - PubMed
-
- Pitt B, Remme W, Zannad F, Neaton J, Martinez F, Roniker B, Bittman R, Hurley S, Kleiman J, Gatlin M. Eplerenone, a selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarction. The New England journal of medicine. 2003;348:1309–1321. - PubMed
-
- Zannad F, McMurray JJ, Krum H, van Veldhuisen DJ, Swedberg K, Shi H, Vincent J, Pocock SJ, Pitt B, Group E-HS. Eplerenone in patients with systolic heart failure and mild symptoms. The New England journal of medicine. 2011;364:11–21.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
