

A neuroradiologist's guide to arterial spin labeling MRI in clinical practice
- PMID: 26351201
- PMCID: PMC4648972
- DOI: 10.1007/s00234-015-1571-z
A neuroradiologist's guide to arterial spin labeling MRI in clinical practice
Abstract
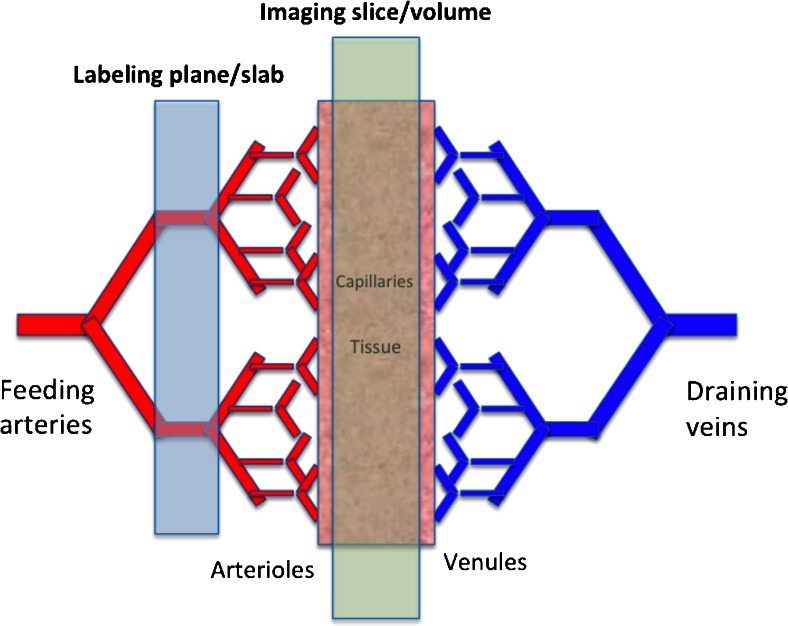
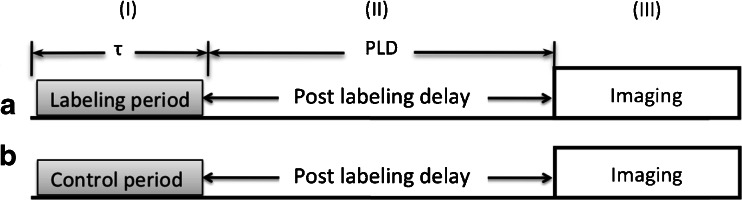
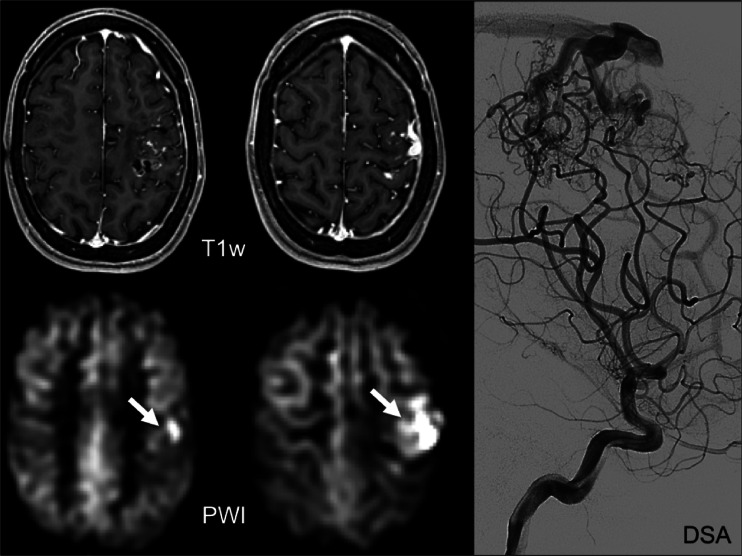
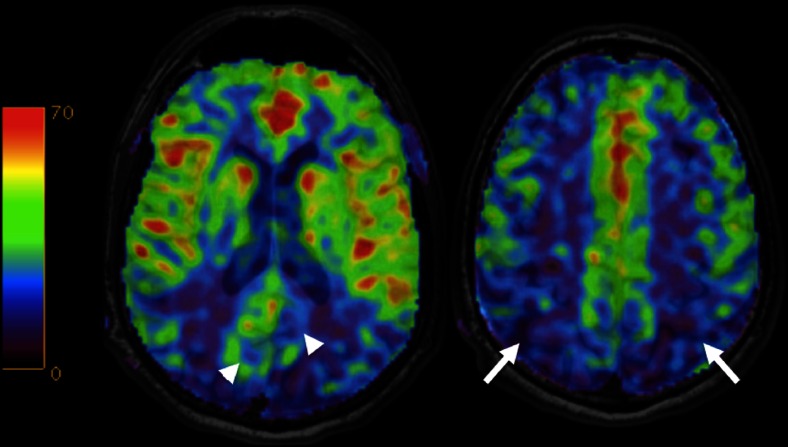
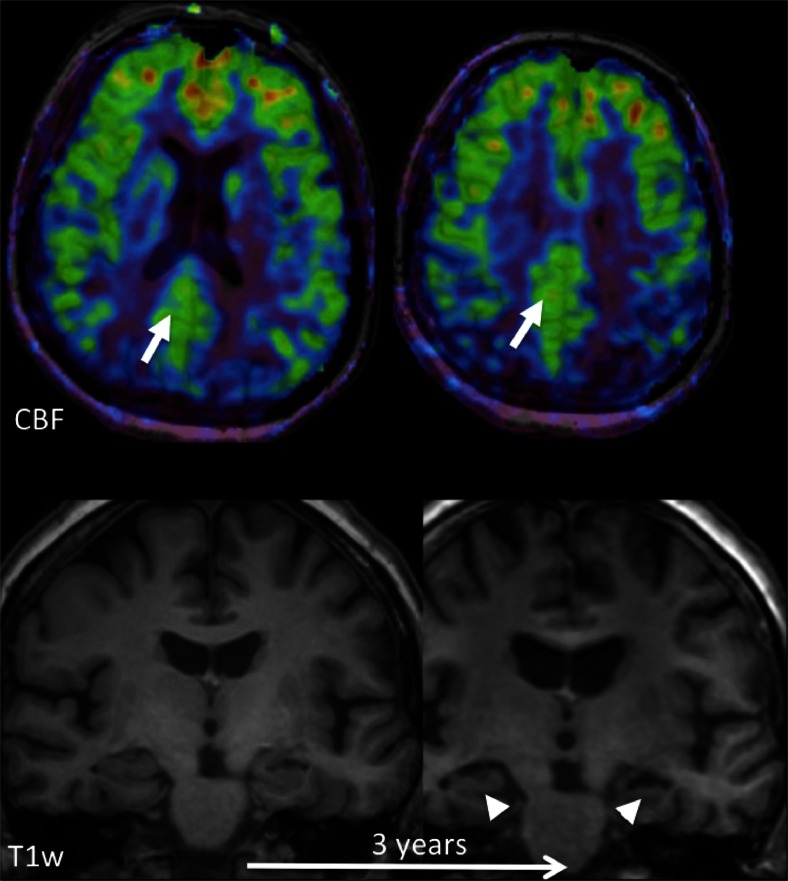
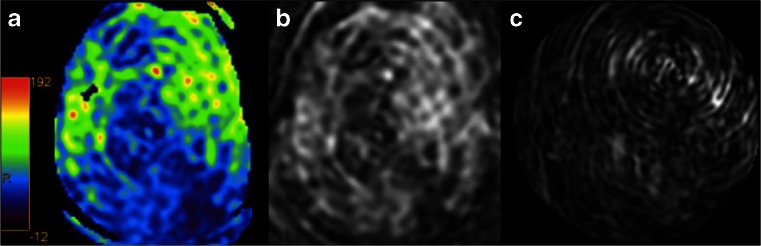
Arterial spin labeling (ASL) is a non-invasive MRI technique to measure cerebral blood flow (CBF). This review provides a practical guide and overview of the clinical applications of ASL of the brain, as well its potential pitfalls. The technical and physiological background is also addressed. At present, main areas of interest are cerebrovascular disease, dementia and neuro-oncology. In cerebrovascular disease, ASL is of particular interest owing to its quantitative nature and its capability to determine cerebral arterial territories. In acute stroke, the source of the collateral blood supply in the penumbra may be visualised. In chronic cerebrovascular disease, the extent and severity of compromised cerebral perfusion can be visualised, which may be used to guide therapeutic or preventative intervention. ASL has potential for the detection and follow-up of arteriovenous malformations. In the workup of dementia patients, ASL is proposed as a diagnostic alternative to PET. It can easily be added to the routinely performed structural MRI examination. In patients with established Alzheimer's disease and frontotemporal dementia, hypoperfusion patterns are seen that are similar to hypometabolism patterns seen with PET. Studies on ASL in brain tumour imaging indicate a high correlation between areas of increased CBF as measured with ASL and increased cerebral blood volume as measured with dynamic susceptibility contrast-enhanced perfusion imaging. Major advantages of ASL for brain tumour imaging are the fact that CBF measurements are not influenced by breakdown of the blood-brain barrier, as well as its quantitative nature, facilitating multicentre and longitudinal studies.
Keywords: Arterial spin labeling; Brain tumour; Dementia; Perfusion; Stroke.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
