

Prognostic Implications of Serum Lipid Metabolism over Time during Sepsis
- PMID: 26351639
- PMCID: PMC4553311
- DOI: 10.1155/2015/789298
Prognostic Implications of Serum Lipid Metabolism over Time during Sepsis
Abstract
Background: Despite extensive research and an improved standard of care, sepsis remains a disorder with a high mortality rate. Sepsis is accompanied by severe metabolic alterations.
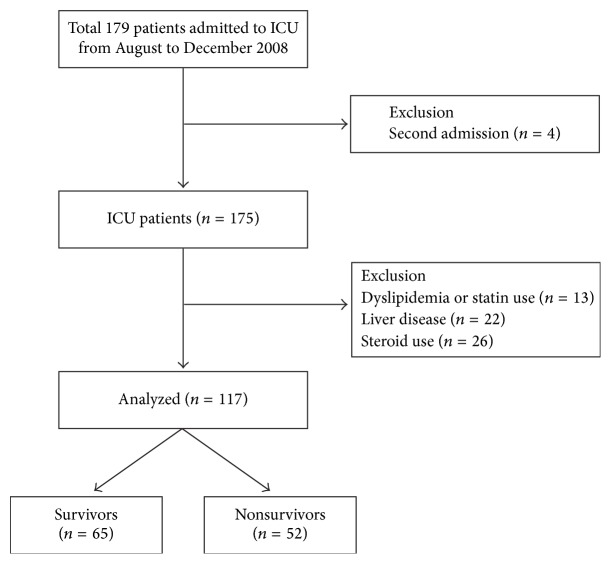
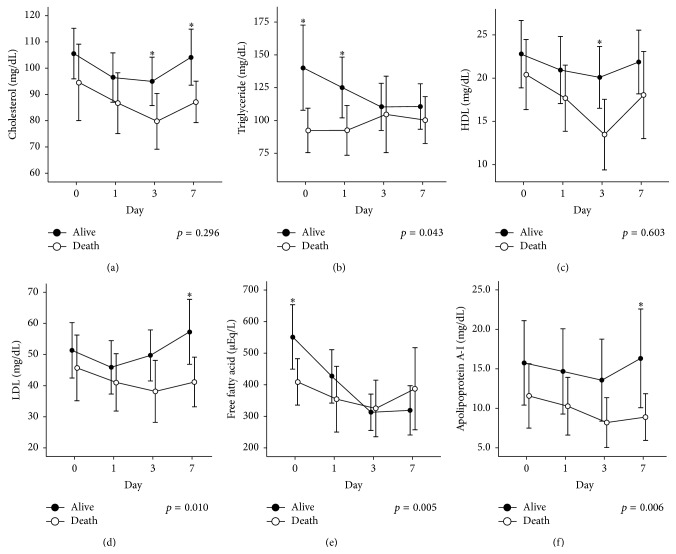
Methods: We evaluated 117 patients with sepsis (severe sepsis [n = 19] and septic shock [n = 98]) who were admitted to the intensive care unit. Serum cholesterol, triglyceride (TG), high-density lipoprotein (HDL), low-density lipoprotein (LDL), free fatty acid (FFA), and apolipoprotein (Apo) A-I levels were measured on days 0, 1, 3, and 7.
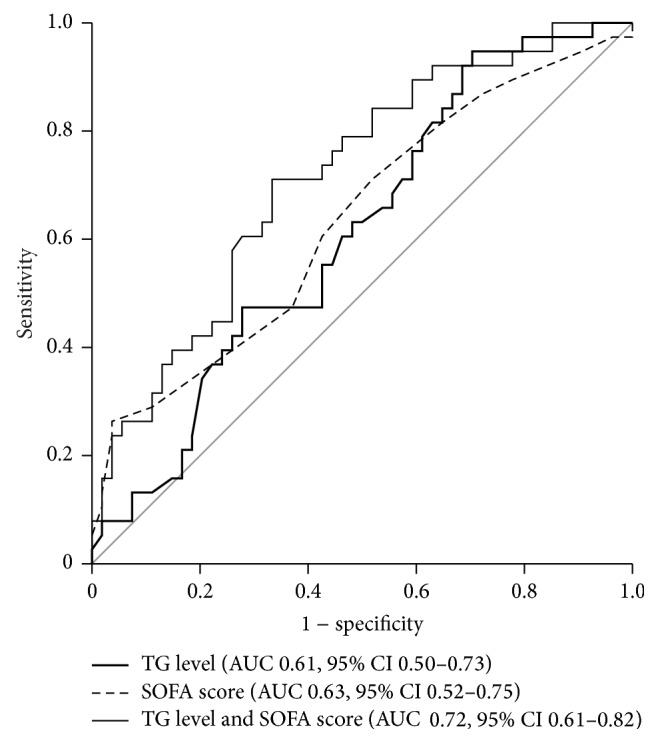
Results: Nonsurvivors had low levels of cholesterol, TG, HDL, LDL, and Apo A-I on days 0, 1, 3, and 7. In a linear mixed model analysis, the variations in TG, LDL, FFA, and Apo A-I levels over time differed significantly between the groups (p = 0.043, p = 0.020, p = 0.005, and p = 0.015, resp.). According to multivariate analysis, TG levels and SOFA scores were associated with mortality on days 0 and 1 (p = 0.018 and p = 0.008, resp.).
Conclusions: Our study illustrated that TG levels are associated with mortality in patients with sepsis. This may be attributable to alterations in serum lipid metabolism during sepsis, thus modulating the host response to inflammation in critically ill patients.
Figures
Similar articles
-
Changes in lipid metabolism in pediatric patients with severe sepsis and septic shock.Nutrition. 2018 Mar;47:104-109. doi: 10.1016/j.nut.2017.09.015. Epub 2017 Oct 12. Nutrition. 2018. PMID: 29429528
-
Serum lipids and disease severity in children with severe meningococcal sepsis.Crit Care Med. 2005 Jul;33(7):1610-5. doi: 10.1097/01.ccm.0000171272.50888.ad. Crit Care Med. 2005. PMID: 16003070
-
Influence of triglyceride concentration on the relationship between lipoprotein cholesterol and apolipoprotein B and A-I levels.Metabolism. 2000 Jan;49(1):53-61. doi: 10.1016/s0026-0495(00)90688-7. Metabolism. 2000. PMID: 10647064 Clinical Trial.
-
Lipid metabolism in critical illness.Curr Opin Clin Nutr Metab Care. 2016 Mar;19(2):111-5. doi: 10.1097/MCO.0000000000000253. Curr Opin Clin Nutr Metab Care. 2016. PMID: 26828580 Review.
-
Lipid profile associated with the systemic inflammatory response syndrome and sepsis in critically ill patients.Nutrition. 2018 Nov;55-56:7-14. doi: 10.1016/j.nut.2018.04.007. Epub 2018 May 9. Nutrition. 2018. PMID: 29960160
Cited by
-
Elevated circulating PCSK9 level is associated with 28-day mortality in patients with sepsis: a prospective cohort study.BMC Emerg Med. 2023 Oct 31;23(1):127. doi: 10.1186/s12873-023-00896-6. BMC Emerg Med. 2023. PMID: 37904138 Free PMC article.
-
The impact of bacteremia on lipoprotein concentrations and patient's outcome: a retrospective analysis.Eur J Clin Microbiol Infect Dis. 2019 Jul;38(7):1279-1286. doi: 10.1007/s10096-019-03543-w. Epub 2019 Apr 13. Eur J Clin Microbiol Infect Dis. 2019. PMID: 30982158 Free PMC article.
-
High-density lipoproteins during sepsis: from bench to bedside.Crit Care. 2020 Apr 7;24(1):134. doi: 10.1186/s13054-020-02860-3. Crit Care. 2020. PMID: 32264946 Free PMC article. Review.
-
Characterising Pre-pubertal Resistance to Death from Endotoxemia.Sci Rep. 2017 Nov 29;7(1):16541. doi: 10.1038/s41598-017-16743-1. Sci Rep. 2017. PMID: 29185479 Free PMC article.
-
U-shaped association between serum triglyceride levels and mortality among septic patients: An analysis based on the MIMIC-IV database.PLoS One. 2023 Nov 27;18(11):e0294779. doi: 10.1371/journal.pone.0294779. eCollection 2023. PLoS One. 2023. PMID: 38011086 Free PMC article.
References
-
- Angus D. C., van der Poll T. Severe sepsis and septic shock. The New England Journal of Medicine. 2013;369(21):p. 2063. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
