

Human cord blood-derived platelet lysate enhances the therapeutic activity of adipose-derived mesenchymal stromal cells isolated from Crohn's disease patients in a mouse model of colitis
- PMID: 26353774
- PMCID: PMC4564981
- DOI: 10.1186/s13287-015-0166-2
Human cord blood-derived platelet lysate enhances the therapeutic activity of adipose-derived mesenchymal stromal cells isolated from Crohn's disease patients in a mouse model of colitis
Abstract
Introduction: Due to their immunomodulatory properties, mesenchymal stromal cells (MSCs) have been used for auto-immune disease treatment. Crohn disease (CD) and ulcerative colitis are two major inflammatory bowel diseases (IBDs), resulting from pathological immune responses to environmental or microbial antigens. Preclinical and clinical studies have suggested that MSC-based cellular therapy hold promising potential for IBD treatment. However, open issues include the selection of the proper cell dose, the source and the optimal route of administration of MSCs for more effective results. Platelet lysate has gained clinical interest due to its efficacy in accelerating wound healing. Thus, we propose to combine the administration of MSCs with a human umbilical cord blood-derived platelet lysate (hCBPL) as a novel strategy to improve MSC-based therapy for IBD resolution.
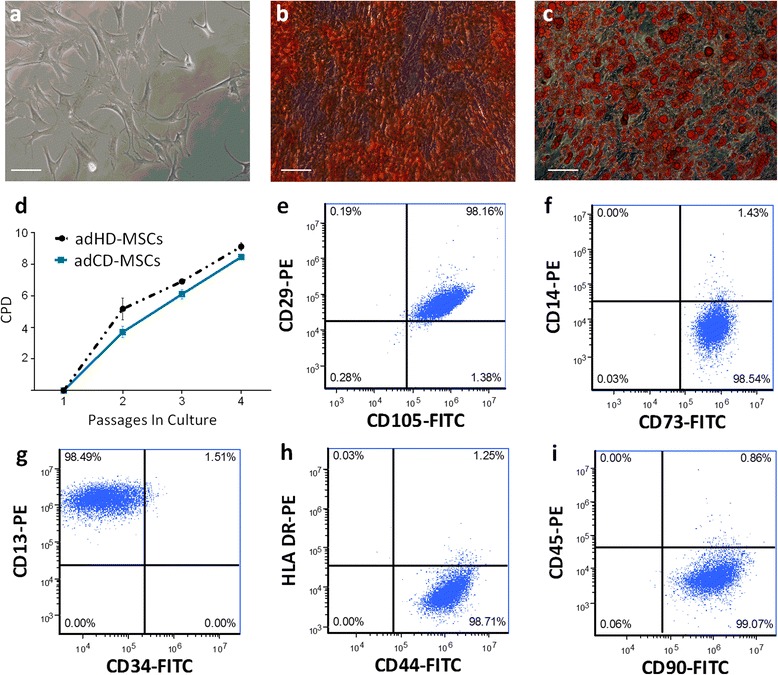
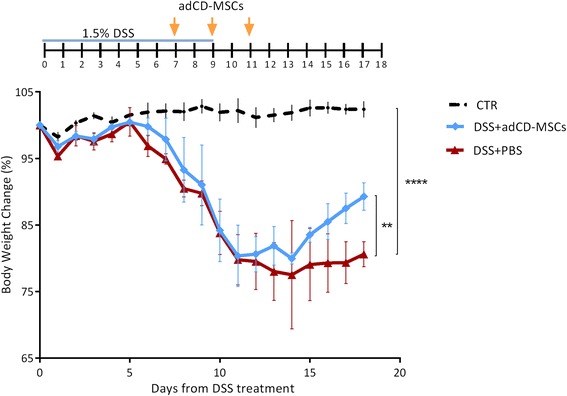
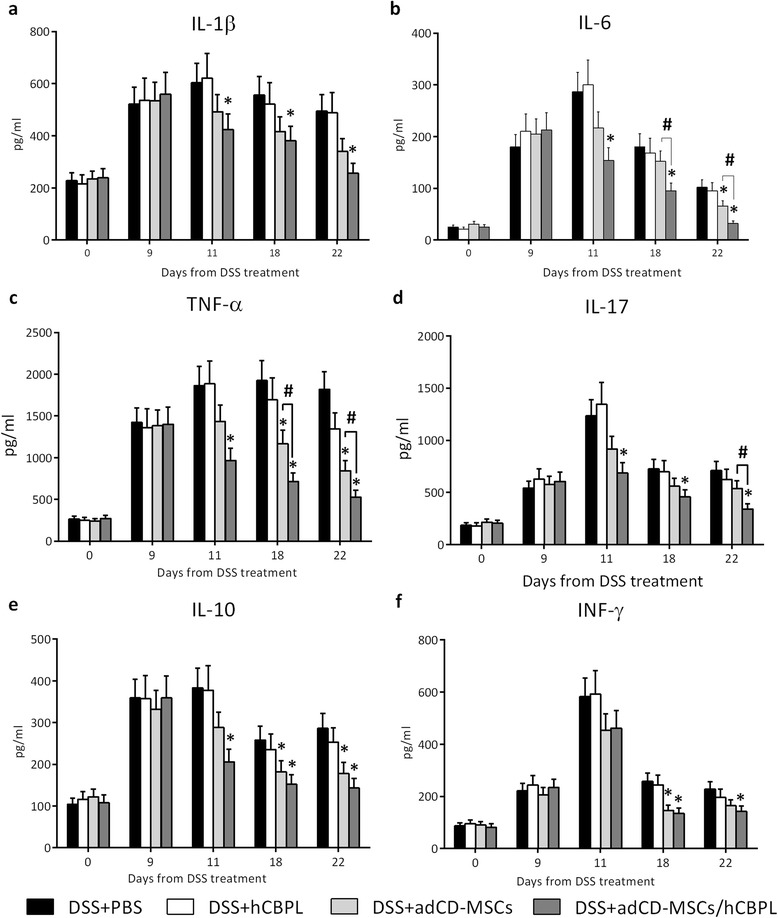
Methods: Colitis was induced in 8-week-old C57BL/6J mice by daily oral administration of dextran sulphate sodium (DSS) (1.5 % w/v in tap water) for 9 days. MSCs were isolated from adipose tissue of CD patients (adCD-MSCs), expanded in proliferation medium, resuspended in hCBPL or PBS and administrated via enema for three times (1 × 10(6) cells/mouse/time) every other day starting on day +7 from DSS induction. The colitis evolution was evaluated by daily monitoring of body weight, stool consistency and bleeding. Histopathological analysis was performed. Inflammatory cytokine plasma levels were determined. adCD-MSCs stained with lipophilic membrane dye Nile Red, were injected in DSS mice as described above. Colon section of mice sacrificed 24 hours after last cell administration, were analyzed by confocal microscopy.
Results: We found that adCD-MSCs could be easily isolated and expanded from CD patients. Upon injection, adCD-MSCs exerted a therapeutic effect on DSS-induced colitis. Moreover, hCBPL increased adCD-MSCs efficacy by significantly reducing colitis scores, extension of the colon inflamed area and plasma levels of inflammatory mediators. Finally, Nile Red staining of MSCs is very efficient, stable and does not impair their vitality and function. Nile Red-labelling was clearly detected in the colitic area of adCD-MSCs injected mice and it was significantly brighter in the colon sections of mice that had received adCD-MSCs/hCBPL.
Conclusions: In summary, with this study we propose a novel and promising adCD-MSC/hCBPL-based therapy for refractory IBDs.
Figures




References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
