Primary Hyperparathyroidism with Extensive Brown Tumors and Multiple Fractures in a 20-Year-Old Woman
- PMID: 26354493
- PMCID: PMC4722419
- DOI: 10.3803/EnM.2015.30.4.614
Primary Hyperparathyroidism with Extensive Brown Tumors and Multiple Fractures in a 20-Year-Old Woman
Abstract
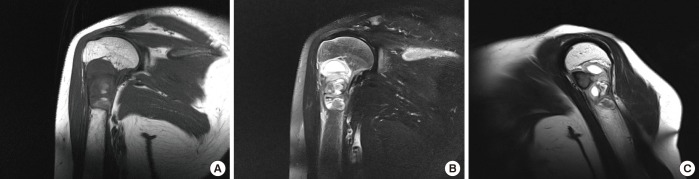
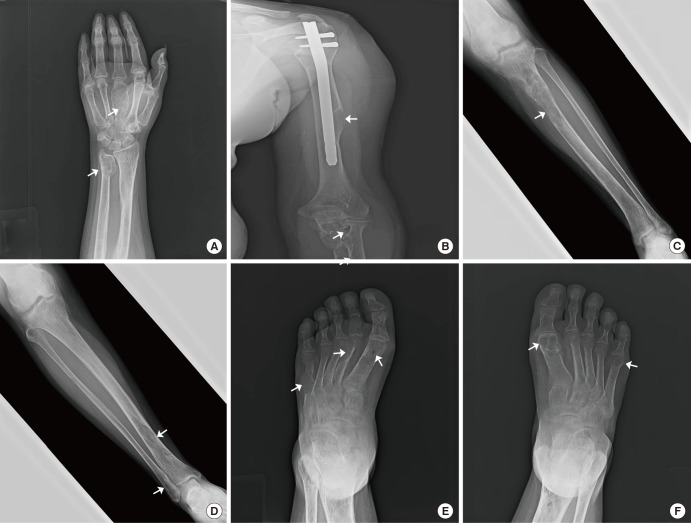
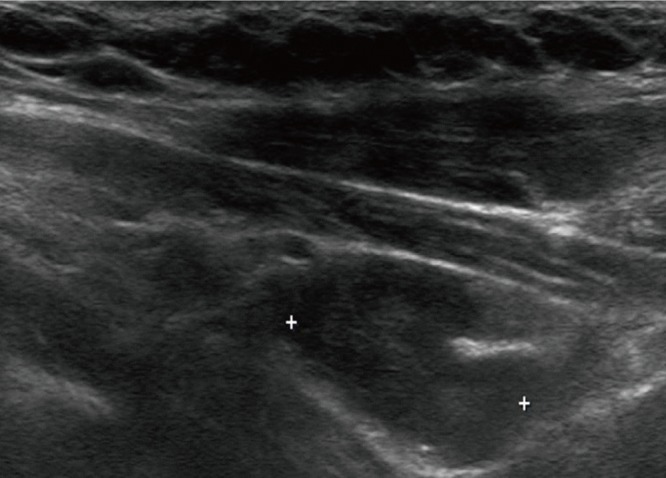
A brown tumor is a benign fibrotic, erosive bony lesion caused by localized, rapid osteoclastic turnover, resulting from hyperparathyroidism. Although brown tumors are one of the most pathognomonic signs of primary hyperparathyroidism, they are rarely seen in clinical practice. In this report, we present a case of 20-year-old woman with recurrent fractures and bone pain. Plain digital radiographs of the affected bones revealed multiple erosive bone tumors, which were finally diagnosed as brown tumors associated with primary hyperparathyroidism due to a parathyroid adenoma. This case shows that multiple, and clinically severe form of brown tumors can even occur in young patients.
Keywords: Brown tumor; Hyperparathyroidism; Parathyroid neoplasms.
Conflict of interest statement
Figures

Similar articles
-
Primary hyperparathyroidism with extensive brown tumours and distal humerus fracture-A case report.Int J Surg Case Rep. 2020;66:421-424. doi: 10.1016/j.ijscr.2019.12.042. Epub 2020 Jan 16. Int J Surg Case Rep. 2020. PMID: 31991305 Free PMC article.
-
Multiple brown tumors in primary hyperparathyroidism.Radiol Case Rep. 2022 Sep 9;17(11):4239-4243. doi: 10.1016/j.radcr.2022.07.110. eCollection 2022 Nov. Radiol Case Rep. 2022. PMID: 36120515 Free PMC article.
-
Calcaneal brown tumor with primary hyperparathyroidism caused by parathyroid carcinoma: an atypical localization.J Foot Ankle Surg. 2004 Jul-Aug;43(4):248-51. doi: 10.1053/j.jfas.2004.05.001. J Foot Ankle Surg. 2004. PMID: 15284814
-
Brown tumors of the jaws associated with primary or secondary hyperparathyroidism. A clinical study and review of the literature.Am J Otolaryngol. 2006 Jul-Aug;27(4):281-6. doi: 10.1016/j.amjoto.2005.11.004. Am J Otolaryngol. 2006. PMID: 16798410 Review.
-
[Multiple maxillofacial brown tumors as primary hyperparathyroidism manifestation].Gac Med Mex. 2008 Mar-Apr;144(2):155-60. Gac Med Mex. 2008. PMID: 18590035 Review. Spanish.
Cited by
-
Bone tumors in the maxilla and the tibia leading to the diagnosis of asymptomatic primary hyperparathyroidism in a 17-year-old male: A case report.Int J Surg Case Rep. 2025 Apr;129:111182. doi: 10.1016/j.ijscr.2025.111182. Epub 2025 Mar 21. Int J Surg Case Rep. 2025. PMID: 40132525 Free PMC article.
-
Gnathic Bones and Hyperparathyroidism: A Review on the Metabolic Bony Changes Affecting the Mandible and Maxilla in case of Hyperparathyroidism.Adv Med. 2020 Jul 9;2020:6836123. doi: 10.1155/2020/6836123. eCollection 2020. Adv Med. 2020. PMID: 32695835 Free PMC article. Review.
-
Utility of 99mTc-Sestamibi SPECT/CT in the Early Localization of Metastatic Parathyroid Carcinoma.Asia Ocean J Nucl Med Biol. 2018 Spring;6(2):171-178. doi: 10.22038/aojnmb.2017.27484.1190. Asia Ocean J Nucl Med Biol. 2018. PMID: 29998152 Free PMC article.
-
Update on brown tumor of hyperparathyroidism.Rev Assoc Med Bras (1992). 2024 Jun 7;70(suppl 1):e2024S132. doi: 10.1590/1806-9282.2024S132. eCollection 2024. Rev Assoc Med Bras (1992). 2024. PMID: 38865551 Free PMC article. No abstract available.
-
Osteolytic Lesions (Brown Tumors) of Primary Hyperparathyroidism: A Report of Two Cases.Cureus. 2024 Jun 5;16(6):e61708. doi: 10.7759/cureus.61708. eCollection 2024 Jun. Cureus. 2024. PMID: 38975429 Free PMC article.
References
-
- Bilezikian JP, Silverberg SJ. Clinical practice. Asymptomatic primary hyperparathyroidism. N Engl J Med. 2004;350:1746–1751. - PubMed
-
- Silverberg SJ, Bilezikian JP. Evaluation and management of primary hyperparathyroidism. J Clin Endocrinol Metab. 1996;81:2036–2040. - PubMed
-
- Keyser JS, Postma GN. Brown tumor of the mandible. Am J Otolaryngol. 1996;17:407–410. - PubMed
-
- Triantafillidou K, Zouloumis L, Karakinaris G, Kalimeras E, Iordanidis F. Brown tumors of the jaws associated with primary or secondary hyperparathyroidism: a clinical study and review of the literature. Am J Otolaryngol. 2006;27:281–286. - PubMed
LinkOut - more resources
Full Text Sources