

Case report of severe Cushing's syndrome in medullary thyroid cancer complicated by functional diabetes insipidus, aortic dissection, jejunal intussusception, and paraneoplastic dysautonomia: remission with sorafenib without reduction in cortisol concentration
- PMID: 26354794
- PMCID: PMC4563835
- DOI: 10.1186/s12885-015-1620-3
Case report of severe Cushing's syndrome in medullary thyroid cancer complicated by functional diabetes insipidus, aortic dissection, jejunal intussusception, and paraneoplastic dysautonomia: remission with sorafenib without reduction in cortisol concentration
Abstract
Background: Normalization of cortisol concentration by multikinase inhibitors have been reported in three patients with medullary thyroid cancer-related Cushing's syndrome. Aortic dissection has been reported in three patients with Cushing's syndrome. Diabetes insipidus without intrasellar metastasis, intestinal intussusception, and paraneoplastic dysautonomia have not been reported in medullary thyroid cancer.
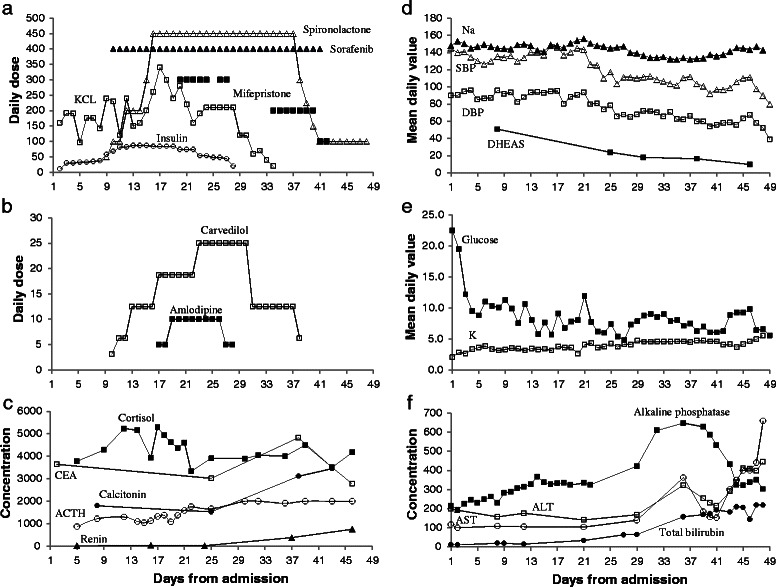
Case presentation: An adult male with metastatic medullary thyroid cancer presented with hyperglycemia, hypernatremia, hypokalemia, hypertension, acne-like rash, and diabetes insipidus (urine volume >8 L/d, osmolality 190 mOsm/kg). Serum cortisol, adrenocorticoitropic hormone, dehydroepiandrostenedione sulfate, and urinary free cortisol were elevated 8, 20, 4.4, and 340 folds, respectively. Pituitary imaging was normal. Computed tomography scan revealed jejunal intussusception and incidental abdominal aortic dissection. Sorafenib treatment was associated with Cushing's syndrome remission, elevated progesterone (>10 fold), normalization of dehydroepiandrostenedione sulfate, but persistently elevated cortisol concentration. Newly-developed proximal lower limb weakness and decreased salivation were associated with elevated ganglionic neuronal acetylcholine receptor (alpha-3) and borderline P/Q type calcium channel antibodies.
Conclusion: Extreme cortisol concentration may have contributed to aortic dissection and suppressed antidiuretic hormone secretion; which combined with hypokalemia due cortisol activation of mineralocorticoid receptors, manifested as diabetes insipidus. This is the first report of paraneoplastic dysautonomia and jejunal intussusception in medullary thyroid cancer, they may be related to medullary thyroid cancer's neuroendocrine origin and metastasis, respectively. Remission of Cushing's syndrome without measurable reduction in cortisol concentration suggests a novel cortisol-independent mechanism of action or assay cross-reactivity. Normalization of dehydroepiandrostenedione sulfate and elevation of progesterone suggest inhibition of 17-hydroxylase and 21-hydroxylase activities by sorafenib.
Figures

References
-
- Isidori AM, Kaltsas GA, Pozza C, Frajese V, Newell-Price J, Reznek RH, Jenkins PJ, Monson JP, Grossman AB, Besser GM. The ectopic adrenocorticotropin syndrome: clinical features, diagnosis, management, and long-term follow up. J Clin Endocrinol Metab. 2006;91(2):371–7. doi: 10.1210/jc.2005-1542. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
