

Resource Utilization and Safety of Outpatient Management Following Intensive Induction or Salvage Chemotherapy for Acute Myeloid Leukemia or Myelodysplastic Syndrome: A Nonrandomized Clinical Comparative Analysis
- PMID: 26355382
- PMCID: PMC4720981
- DOI: 10.1001/jamaoncol.2015.2969
Resource Utilization and Safety of Outpatient Management Following Intensive Induction or Salvage Chemotherapy for Acute Myeloid Leukemia or Myelodysplastic Syndrome: A Nonrandomized Clinical Comparative Analysis
Abstract
Importance: Adults with acute myeloid leukemia (AML) or myelodysplastic syndrome (MDS) typically remain hospitalized after induction or salvage chemotherapy until blood cell count recovery, with resulting prolonged inpatient stays being a primary driver of health care costs. Pilot studies suggest that outpatient management following chemotherapy might be safe and could reduce costs for these patients.
Objective: To compare safety, resource utilization, infections, and costs between adults discharged early following AML or MDS induction or salvage chemotherapy and inpatient controls.
Design: Nonrandomized, phase 2, single-center study conducted at the University of Washington Medical Center. Over a 43-month period (January 1, 2011, through July 31, 2014), 178 adults receiving intensive AML or MDS chemotherapy were enrolled. After completion of chemotherapy, 107 patients met predesignated medical and logistical criteria for early discharge, while 29 met medical criteria only and served as inpatient controls.
Interventions: Early-discharge patients were released from the hospital at the completion of chemotherapy, and supportive care was provided in the outpatient setting until blood cell count recovery (median, 21 days; range, 2-45 days). Controls received inpatient supportive care (median, 16 days; range, 3-42 days).
Main outcomes and measures: We analyzed differences in early mortality, resource utilization including intensive care unit (ICU) days, transfusions per study day, and use of intravenous (IV) antibiotics per study day), numbers of infections, and total and inpatient charges per study day among early-discharge patients vs controls.
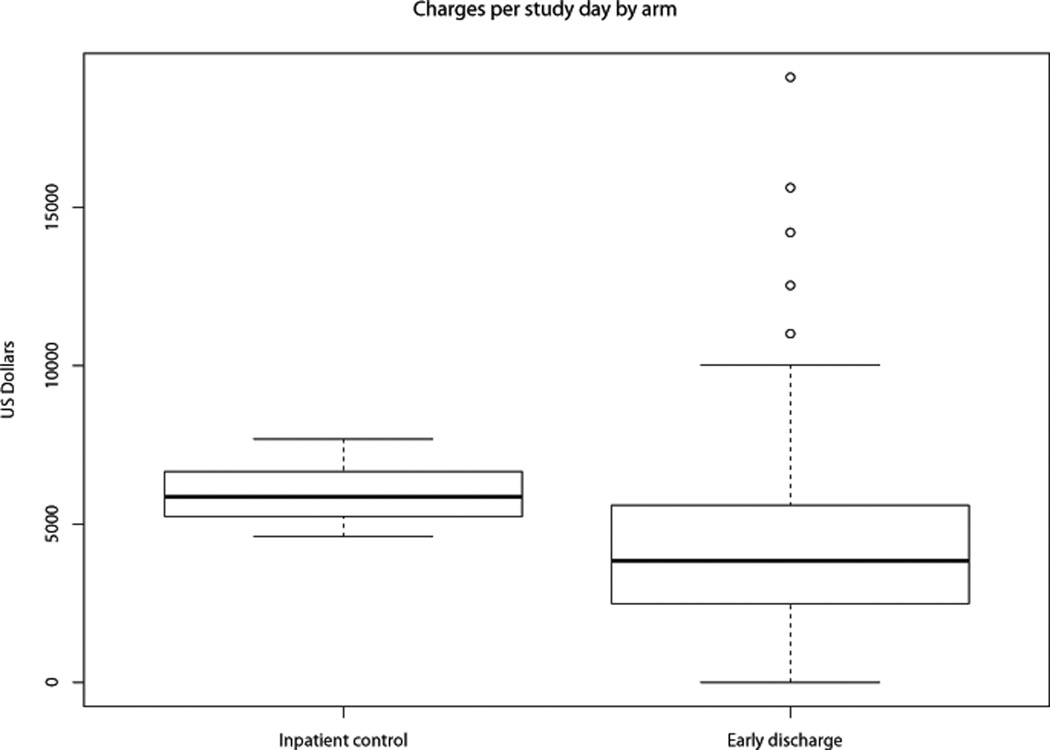
Results: Four of the 107 early-discharge patients and none of the 29 control patients died within 30 days of enrollment (P=.58). Nine early-discharge patients (8%) but no controls required ICU-level care (P=.20). No differences were noted in the median daily number of transfused red blood cell units (0.27 vs 0.29; P=.55) or number of transfused platelet units (0.26 vs 0.29; P=.31). Early-discharge patients had more positive blood cultures (37 [35%] vs 4 [14%]; P=.04) but required fewer IV antibiotic days per study day (0.48 vs 0.71; P=.01). Overall, daily charges among early-discharge patients were significantly lower than for inpatients (median, $3840 vs $5852; P<.001) despite increased charges per inpatient day when readmitted (median, $7405 vs $5852; P<.001).
Conclusions and relevance: Early discharge following intensive AML or MDS chemotherapy can reduce costs and use of IV antibiotics, but attention should be paid to complications that may occur in the outpatient setting.
Conflict of interest statement
Figures
Similar articles
-
Outpatient management following intensive induction chemotherapy for myelodysplastic syndromes and acute myeloid leukemia: a pilot study.Haematologica. 2011 Jun;96(6):914-7. doi: 10.3324/haematol.2011.040220. Epub 2011 Mar 10. Haematologica. 2011. PMID: 21393334 Free PMC article. Clinical Trial.
-
A comparison of resource utilization following chemotherapy for acute myeloid leukemia in children discharged versus children that remain hospitalized during neutropenia.Cancer Med. 2015 Sep;4(9):1356-64. doi: 10.1002/cam4.481. Epub 2015 Jun 24. Cancer Med. 2015. PMID: 26105201 Free PMC article.
-
Health economic impact of high-dose versus standard-dose cytarabine induction chemotherapy for acute myeloid leukaemia.Intern Med J. 2014 Aug;44(8):757-63. doi: 10.1111/imj.12478. Intern Med J. 2014. PMID: 24863325
-
Azacitidine for the treatment of myelodysplastic syndrome, chronic myelomonocytic leukaemia and acute myeloid leukaemia.Health Technol Assess. 2010 May;14 Suppl 1:69-74. doi: 10.3310/hta14Suppl1/10. Health Technol Assess. 2010. PMID: 20507806 Review.
-
Outpatient care of patients with acute myeloid leukemia: Benefits, barriers, and future considerations.Leuk Res. 2016 Jun;45:53-8. doi: 10.1016/j.leukres.2016.03.011. Epub 2016 Apr 1. Leuk Res. 2016. PMID: 27101148 Free PMC article. Review.
Cited by
-
Safety and Feasibility of Outpatient High Dose Cytarabine for Acute Myeloid Leukemia in the Brazilian Amazon.Int J Hematol Oncol Stem Cell Res. 2020 Jul 1;14(3):151-156. doi: 10.18502/ijhoscr.v14i3.3722. Int J Hematol Oncol Stem Cell Res. 2020. PMID: 33024520 Free PMC article.
-
Healthcare resource utilization trends in patients with acute myeloid leukemia ineligible for intensive chemotherapy receiving first-line systemic treatment or best supportive care: A multicenter international study.Eur J Haematol. 2022 Jul;109(1):58-68. doi: 10.1111/ejh.13769. Epub 2022 Apr 13. Eur J Haematol. 2022. PMID: 35298049 Free PMC article.
-
CPX-351: a nanoscale liposomal co-formulation of daunorubicin and cytarabine with unique biodistribution and tumor cell uptake properties.Int J Nanomedicine. 2019 May 23;14:3819-3830. doi: 10.2147/IJN.S139450. eCollection 2019. Int J Nanomedicine. 2019. PMID: 31213803 Free PMC article. Review.
-
Factors and Costs Associated With Delay in Treatment Initiation and Prolonged Length of Stay With Inpatient EPOCH Chemotherapy in Patients With Hematologic Malignancies.Cancer Invest. 2017 Mar 16;35(3):202-214. doi: 10.1080/07357907.2016.1276186. Epub 2017 Feb 6. Cancer Invest. 2017. PMID: 28165774 Free PMC article.
-
Access to Therapy for Acute Myeloid Leukemia in the Developing World: Barriers and Solutions.Curr Oncol Rep. 2020 Oct 6;22(12):125. doi: 10.1007/s11912-020-00987-8. Curr Oncol Rep. 2020. PMID: 33025161 Free PMC article. Review.
References
-
- Ferrara F, Schiffer CA. Acute myeloid leukaemia in adults. Lancet. 2013;381(9865):484–495. - PubMed
-
- Ades L, Itzykson R, Fenaux P. Myelodysplastic syndromes. Lancet. 2014;383(9936):2239–2252. - PubMed
-
- Redaelli A, Botteman MF, Stephens JM, Brandt S, Pashos CL. Economic burden of acute myeloid leukemia: a literature review. Cancer Treat Rev. 2004;30(3):237–247. - PubMed
-
- Nerich V, Lioure B, Rave M, et al. Induction-related cost of patients with acute myeloid leukaemia in France. Int J Clin Pharm. 2011;33(2):191–199. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
