

Accuracy of Patient Self-Report of Stroke: A Systematic Review from the UK Biobank Stroke Outcomes Group
- PMID: 26355837
- PMCID: PMC4565695
- DOI: 10.1371/journal.pone.0137538
Accuracy of Patient Self-Report of Stroke: A Systematic Review from the UK Biobank Stroke Outcomes Group
Abstract
Objective: We performed a systematic review of the accuracy of patient self-report of stroke to inform approaches to ascertaining and confirming stroke cases in large prospective studies.
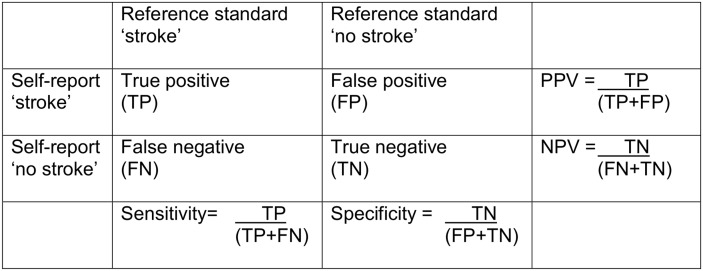
Methods: We sought studies comparing patient self-report against a reference standard for stroke. We extracted data on survey method(s), response rates, participant characteristics, the reference standard used, and the positive predictive value (PPV) of self-report. Where possible we also calculated sensitivity, specificity, negative predictive value (NPV), and stroke prevalence. Study-level risk of bias was assessed using the Quality Assessment of Diagnostic Studies tool (QUADAS-2).
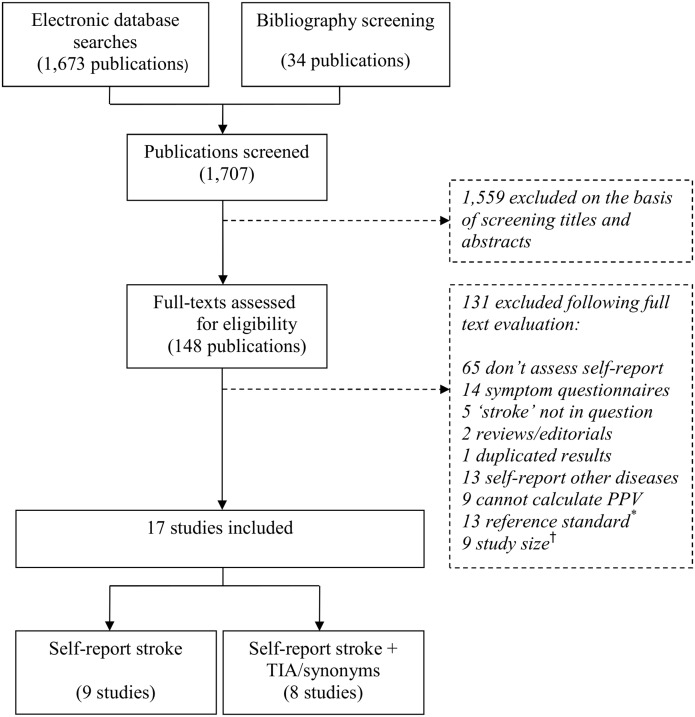
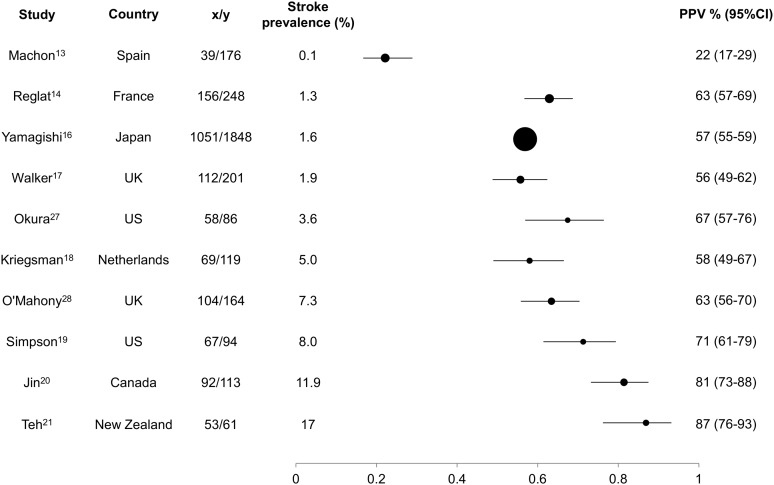
Results: From >1500 identified articles, we included 17 studies. Most asked patients to report a lifetime history of stroke but a few limited recall time to ≤5 years. Some included questions for transient ischaemic attack (TIA) or stroke synonyms. No study was free of risk of bias in the QUADAS-2 assessment, the most frequent causes of bias being incomplete reference standard data, absence of blinding of adjudicators to self-report status, and participant response rates (<80%). PPV of self-report ranged from 22-87% (17 studies), sensitivity from 36-98% (10 studies), specificity from 96-99.6% (10 studies), and NPV from 88.2-99.9% (10 studies). PPV increased with stroke prevalence as expected. Among six studies with available relevant data, if confirmed TIAs were considered to be true rather than false positive strokes, PPV of self-report was >75% in all but one study. It was not possible to assess the influence of recall time or of the question(s) asked on PPV or sensitivity.
Conclusions: Characteristics of the study population strongly influence self-report accuracy. In population-based studies with low stroke prevalence, a large proportion of self-reported strokes may be false positives. Self-report is therefore unlikely to be helpful for identifying cases without subsequent confirmation, but may be useful for case ascertainment in combination with other data sources.
Conflict of interest statement
Figures
References
-
- Available: http://www.ukbiobank.ac.uk.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
