

Clinical Epidemiology of Buruli Ulcer from Benin (2005-2013): Effect of Time-Delay to Diagnosis on Clinical Forms and Severe Phenotypes
- PMID: 26355838
- PMCID: PMC4565642
- DOI: 10.1371/journal.pntd.0004005
Clinical Epidemiology of Buruli Ulcer from Benin (2005-2013): Effect of Time-Delay to Diagnosis on Clinical Forms and Severe Phenotypes
Abstract
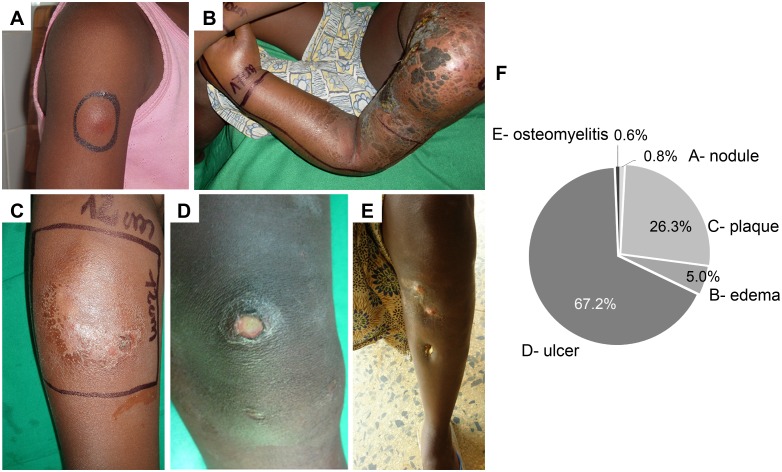
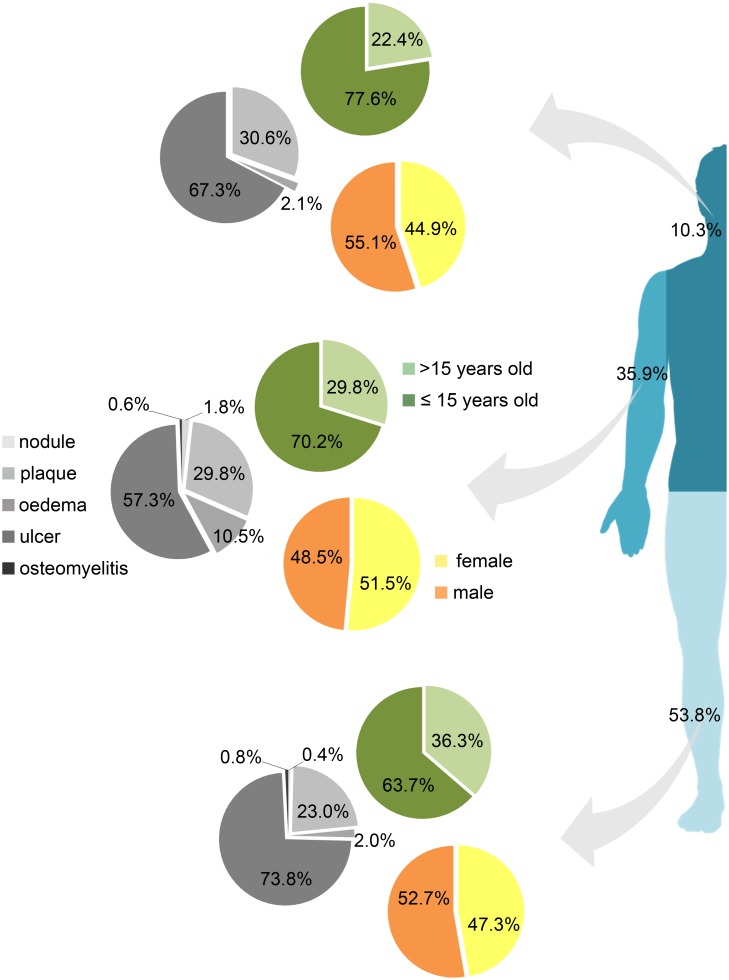
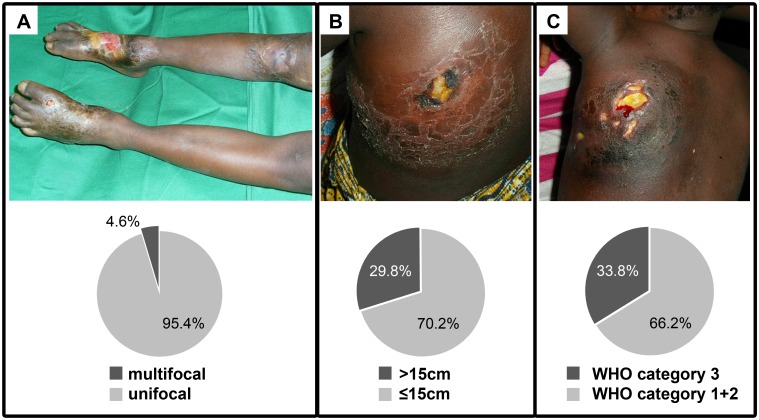
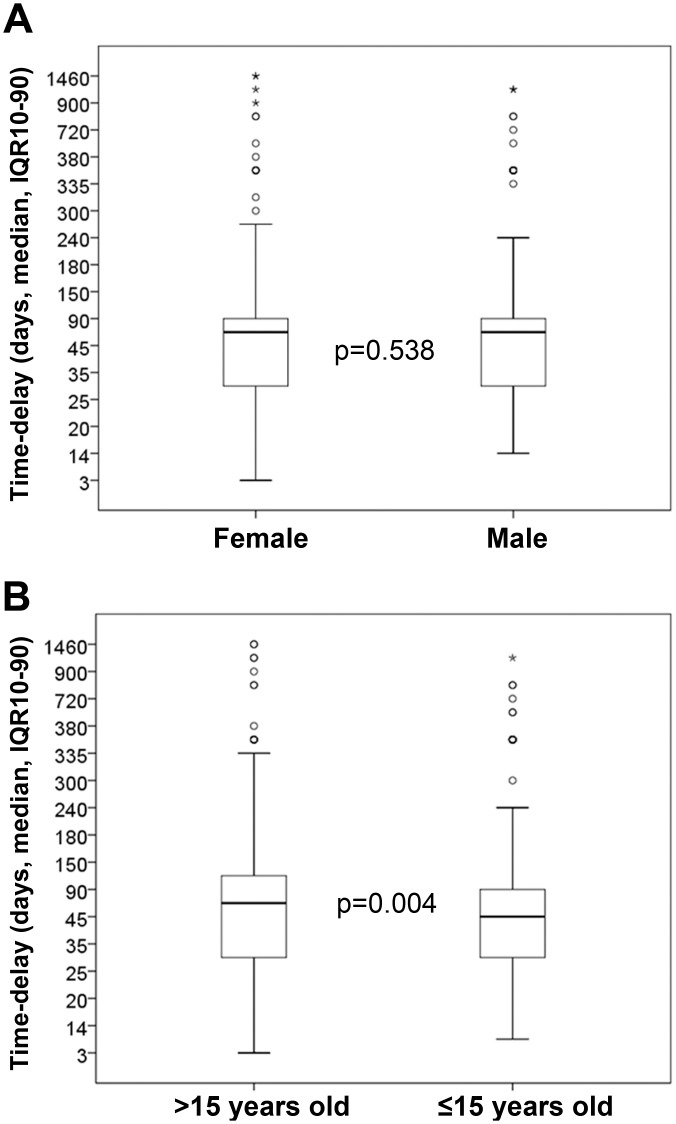
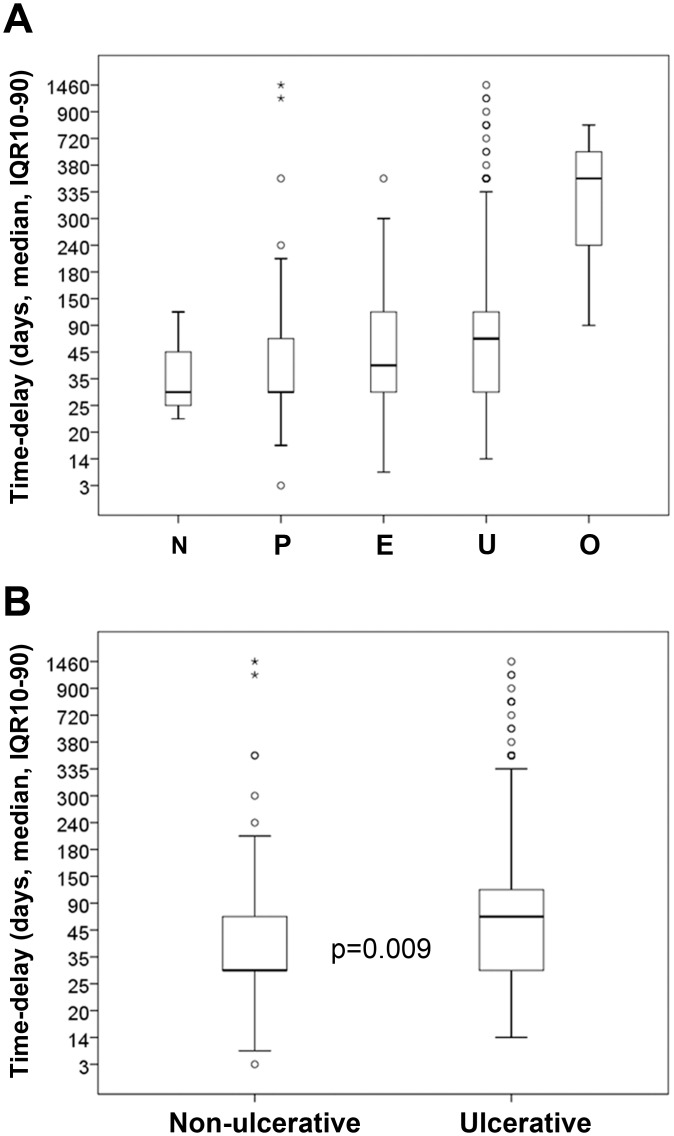
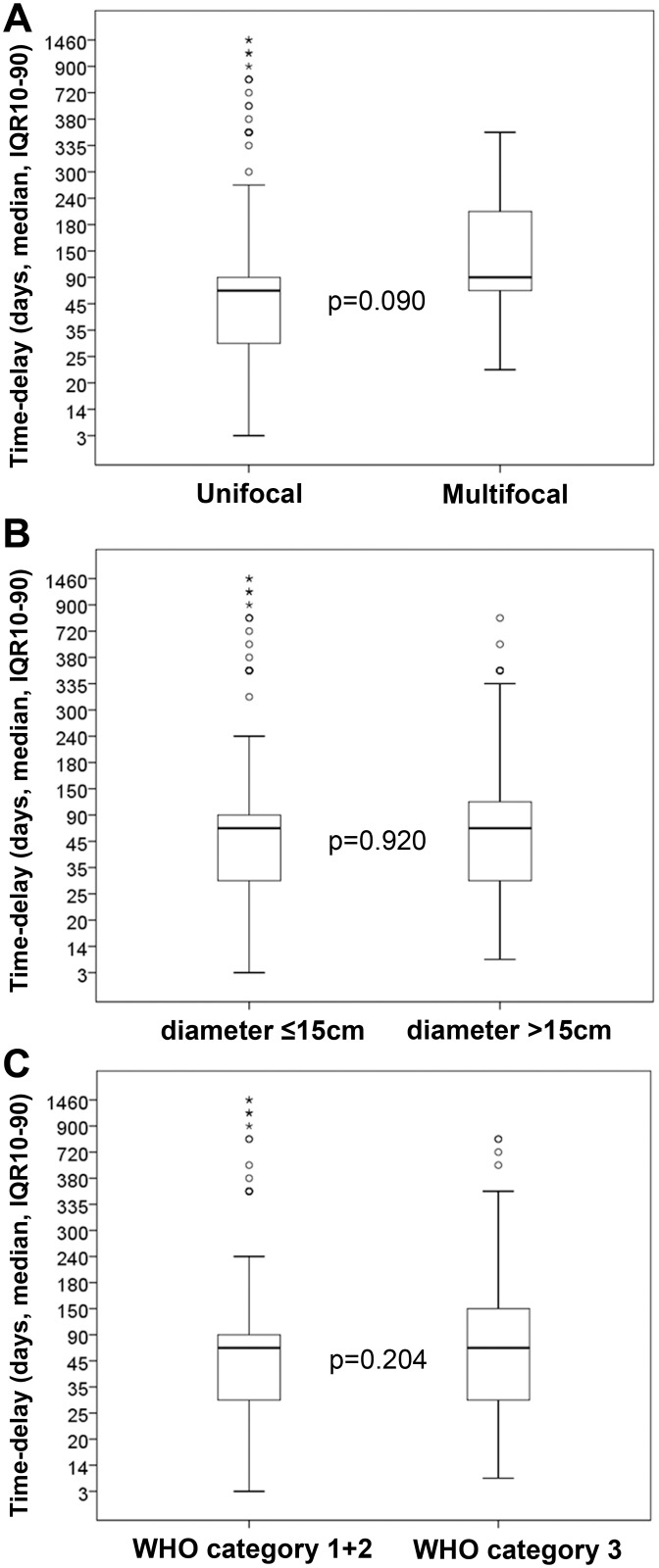
Buruli Ulcer (BU) is a neglected infectious disease caused by Mycobacterium ulcerans that is responsible for severe necrotizing cutaneous lesions that may be associated with bone involvement. Clinical presentations of BU lesions are classically classified as papules, nodules, plaques and edematous infiltration, ulcer or osteomyelitis. Within these different clinical forms, lesions can be further classified as severe forms based on focality (multiple lesions), lesions' size (>15 cm diameter) or WHO Category (WHO Category 3 lesions). There are studies reporting an association between delay in seeking medical care and the development of ulcerative forms of BU or osteomyelitis, but the effect of time-delay on the emergence of lesions classified as severe has not been addressed. To address both issues, and in a cohort of laboratory-confirmed BU cases, 476 patients from a medical center in Allada, Benin, were studied. In this laboratory-confirmed cohort, we validated previous observations, demonstrating that time-delay is statistically related to the clinical form of BU. Indeed, for non-ulcerated forms (nodule, edema, and plaque) the median time-delay was 32.5 days (IQR 30.0-67.5), while for ulcerated forms it was 60 days (IQR 20.0-120.0) (p = 0.009), and for bone lesions, 365 days (IQR 228.0-548.0). On the other hand, we show here that time-delay is not associated with the more severe phenotypes of BU, such as multi-focal lesions (median 90 days; IQR 56-217.5; p = 0.09), larger lesions (diameter >15 cm) (median 60 days; IQR 30-120; p = 0.92) or category 3 WHO classification (median 60 days; IQR 30-150; p = 0.20), when compared with unifocal (median 60 days; IQR 30-90), small lesions (diameter ≤15 cm) (median 60 days; IQR 30-90), or WHO category 1+2 lesions (median 60 days; IQR 30-90), respectively. Our results demonstrate that after an initial period of progression towards ulceration or bone involvement, BU lesions become stable regarding size and focal/multi-focal progression. Therefore, in future studies on BU epidemiology, severe clinical forms should be systematically considered as distinct phenotypes of the same disease and thus subjected to specific risk factor investigation.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Clinical epidemiology of laboratory-confirmed Buruli ulcer in Benin: a cohort study.Lancet Glob Health. 2014 Jul;2(7):e422-30. doi: 10.1016/S2214-109X(14)70223-2. Epub 2014 Jun 17. Lancet Glob Health. 2014. PMID: 25103396
-
Findings in patients from Benin with osteomyelitis and polymerase chain reaction-confirmed Mycobacterium ulcerans infection.Clin Infect Dis. 2014 Nov 1;59(9):1256-64. doi: 10.1093/cid/ciu584. Epub 2014 Jul 21. Clin Infect Dis. 2014. PMID: 25048846
-
Report of a series of 82 cases of Buruli ulcer from Nigeria treated in Benin, from 2006 to 2016.PLoS Negl Trop Dis. 2018 Mar 9;12(3):e0006358. doi: 10.1371/journal.pntd.0006358. eCollection 2018 Mar. PLoS Negl Trop Dis. 2018. PMID: 29522516 Free PMC article.
-
Epidemiology of Buruli Ulcer in Victoria, Australia, 2017-2022.Emerg Infect Dis. 2025 Mar;31(3):448-457. doi: 10.3201/eid3103.240938. Emerg Infect Dis. 2025. PMID: 40023793 Free PMC article. Review.
-
Buruli ulcer (Mycobacterium ulcerans infection).Trans R Soc Trop Med Hyg. 2008 Oct;102(10):969-78. doi: 10.1016/j.trstmh.2008.06.006. Epub 2008 Jul 26. Trans R Soc Trop Med Hyg. 2008. PMID: 18657836 Review.
Cited by
-
Genetic Variation in Autophagy-Related Genes Influences the Risk and Phenotype of Buruli Ulcer.PLoS Negl Trop Dis. 2016 Apr 29;10(4):e0004671. doi: 10.1371/journal.pntd.0004671. eCollection 2016 Apr. PLoS Negl Trop Dis. 2016. PMID: 27128681 Free PMC article.
-
The immunology of other mycobacteria: M. ulcerans, M. leprae.Semin Immunopathol. 2020 Jun;42(3):333-353. doi: 10.1007/s00281-020-00790-4. Epub 2020 Feb 25. Semin Immunopathol. 2020. PMID: 32100087 Free PMC article. Review.
-
Delays in Patient Presentation and Diagnosis for Buruli Ulcer (Mycobacterium ulcerans Infection) in Victoria, Australia, 2011-2017.Trop Med Infect Dis. 2019 Jul 4;4(3):100. doi: 10.3390/tropicalmed4030100. Trop Med Infect Dis. 2019. PMID: 31277453 Free PMC article.
-
Infiltrating leukocytes surround early Buruli ulcer lesions, but are unable to reach the mycolactone producing mycobacteria.Virulence. 2017 Nov 17;8(8):1918-1926. doi: 10.1080/21505594.2017.1370530. Epub 2017 Oct 5. Virulence. 2017. PMID: 28873327 Free PMC article. No abstract available.
-
Steps Toward Creating A Therapeutic Community for Inpatients Suffering from Chronic Ulcers: Lessons from Allada Buruli Ulcer Treatment Hospital in Benin.PLoS Negl Trop Dis. 2016 Jul 1;10(7):e0004602. doi: 10.1371/journal.pntd.0004602. eCollection 2016 Jul. PLoS Negl Trop Dis. 2016. PMID: 27367809 Free PMC article.
References
-
- George KM, Chatterjee D, Gunawardana G, Welty D, Hayman J, et al. (1999) Mycolactone: a polyketide toxin from Mycobacterium ulcerans required for virulence. Science 283: 854–857. - PubMed
-
- Boleira M, Lupi O, Lehman L, Asiedu KB, Kiszewski AE (2010) Buruli ulcer. An Bras Dermatol 85: 281–298; quiz 299–301. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
