

The investigation and treatment of female pelvic floor dysfunction
- PMID: 26356560
- PMCID: PMC4570968
- DOI: 10.3238/arztebl.2015.0564
The investigation and treatment of female pelvic floor dysfunction
Abstract
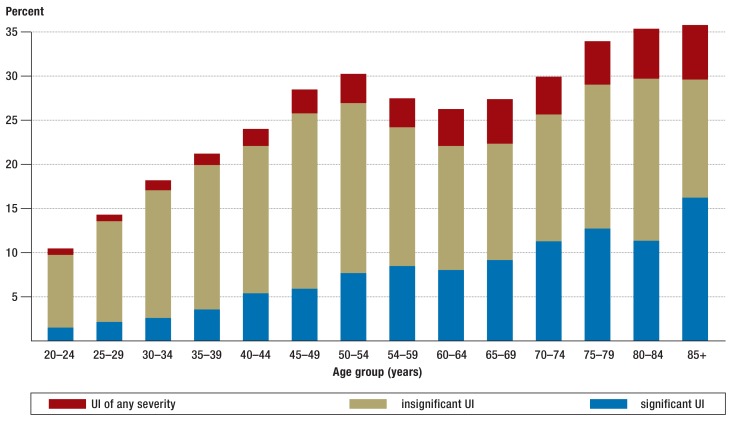
Background: 25% of all women report involuntary loss of urine, and 7% may require treatment.
Methods: This review is based on a selection of pertinent literature, including guidelines and Cochrane reviews.
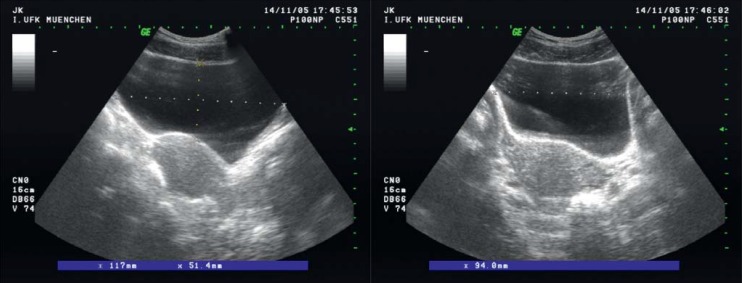
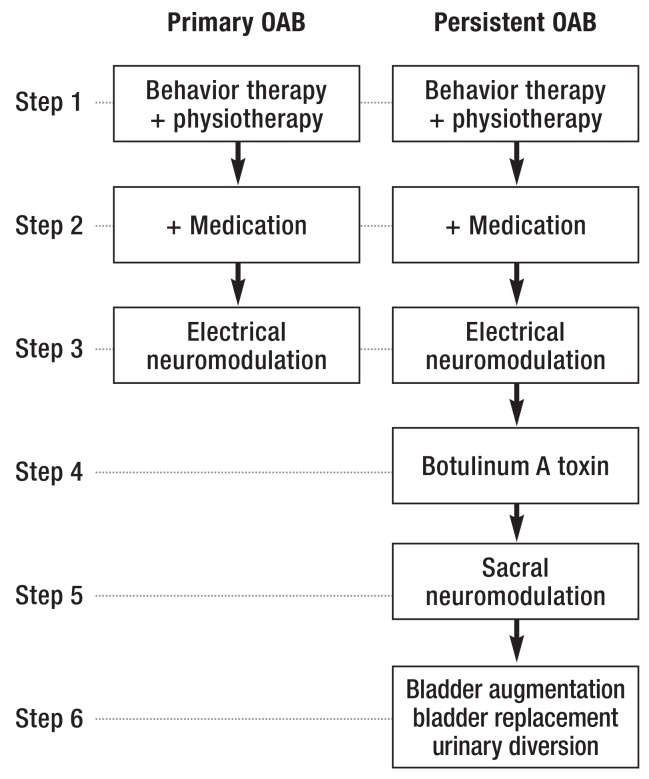
Results: The assessment of pelvic floor dysfunction in women begins with a basic evaluation that is followed by special diagnostic tests if indicated. The physician taking the clinical history should inquire about the patient's behavior, personality, social and other stressors, and eating and drinking habits, as well as any mental disorders that may be present, including anxiety disorders, depression, somatization disorders, and disorders of adaptation. Conservative treatment consists mainly of lifestyle changes, physiotherapy, and medication. Stress incontinence is most commonly treated with pelvic floor exercises, with a documented success rate of 56.1% vs. 6% without such treatment (relative risk 8.38, 95% confidence interval 3.67-19.07). If incontinence persists, surgery may be indicated ( implantation of suburethral tension-free slings, or colposuspension). Feedback and biofeedback training can be used to treat an overactive bladder. If these techniques and drug therapy are unsuccessful, botulinum toxin injections can be considered.
Conclusion: Well-validated treatments for pelvic floor dysfunction are available. Psychosomatic factors must be taken into account and can have a major effect on treatment outcomes.
Figures


Comment in
-
Proctologists Omitted.Dtsch Arztebl Int. 2016 Mar 25;113(12):211. doi: 10.3238/arztebl.2016.0011a. Dtsch Arztebl Int. 2016. PMID: 27118719 Free PMC article. No abstract available.
-
Broadened View.Dtsch Arztebl Int. 2016 Mar 25;113(12):211. doi: 10.3238/arztebl.2016.0011b. Dtsch Arztebl Int. 2016. PMID: 27118720 Free PMC article. No abstract available.
-
Vaginal Delivery as Leading Risk Factor.Dtsch Arztebl Int. 2016 Mar 25;113(12):211-2. doi: 10.3238/arztebl.2016.0011c. Dtsch Arztebl Int. 2016. PMID: 27118721 Free PMC article. No abstract available.
-
NPH Among the Potential Causes.Dtsch Arztebl Int. 2016 Mar 25;113(12):212. doi: 10.3238/arztebl.2016.0012a. Dtsch Arztebl Int. 2016. PMID: 27118722 Free PMC article. No abstract available.
-
In Reply.Dtsch Arztebl Int. 2016 Mar 25;113(12):212. doi: 10.3238/arztebl.2016.0012b. Dtsch Arztebl Int. 2016. PMID: 27118723 Free PMC article. No abstract available.
References
-
- Harninkontinenz. Gesundheitsberichterstattung des Bundes. Robert-Koch-Institut. 2007;Band 39
-
- Abrams P, Cardozo L, Fall M, et al. The standardisation of terminology of lower urinary tract function: Report from the Standardisation Subcommittee of the International Continence Society. Neurourol Urodyn. 2002;21(2):167–178. - PubMed
-
- Hannestad YS, Rortveit G, Sandvik H, et al. A community-based epidemiological survey of female urinary incontinence: The Norwegian EPINCONT Study. J Clin Epidemiol. 2000;53:1150–1157. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical