

Spinal Dural Arteriovenous Fistula: Imaging Features and Its Mimics
- PMID: 26357504
- PMCID: PMC4559784
- DOI: 10.3348/kjr.2015.16.5.1119
Spinal Dural Arteriovenous Fistula: Imaging Features and Its Mimics
Abstract
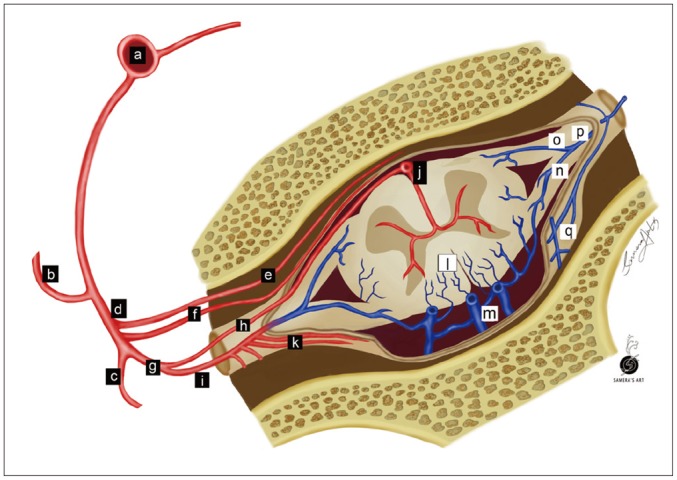
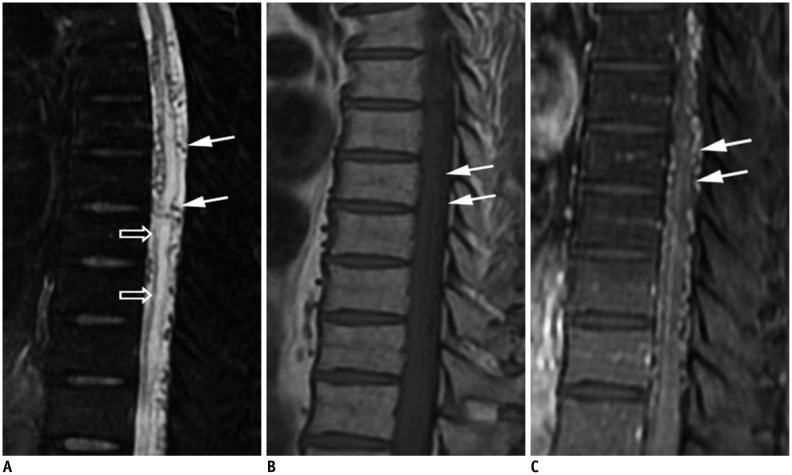
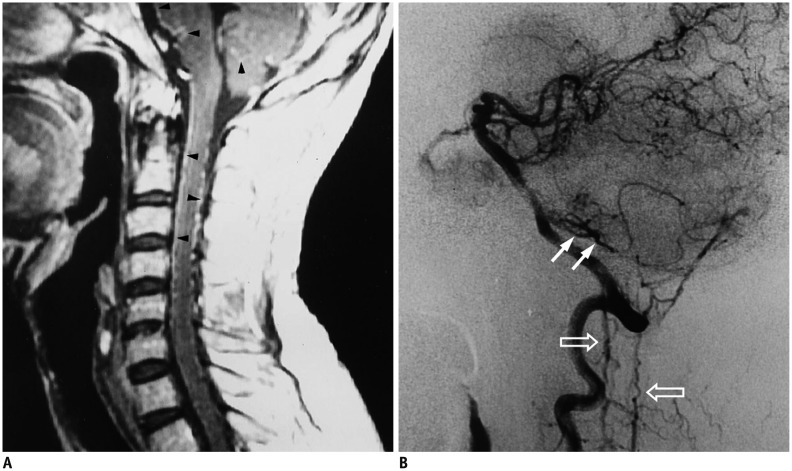
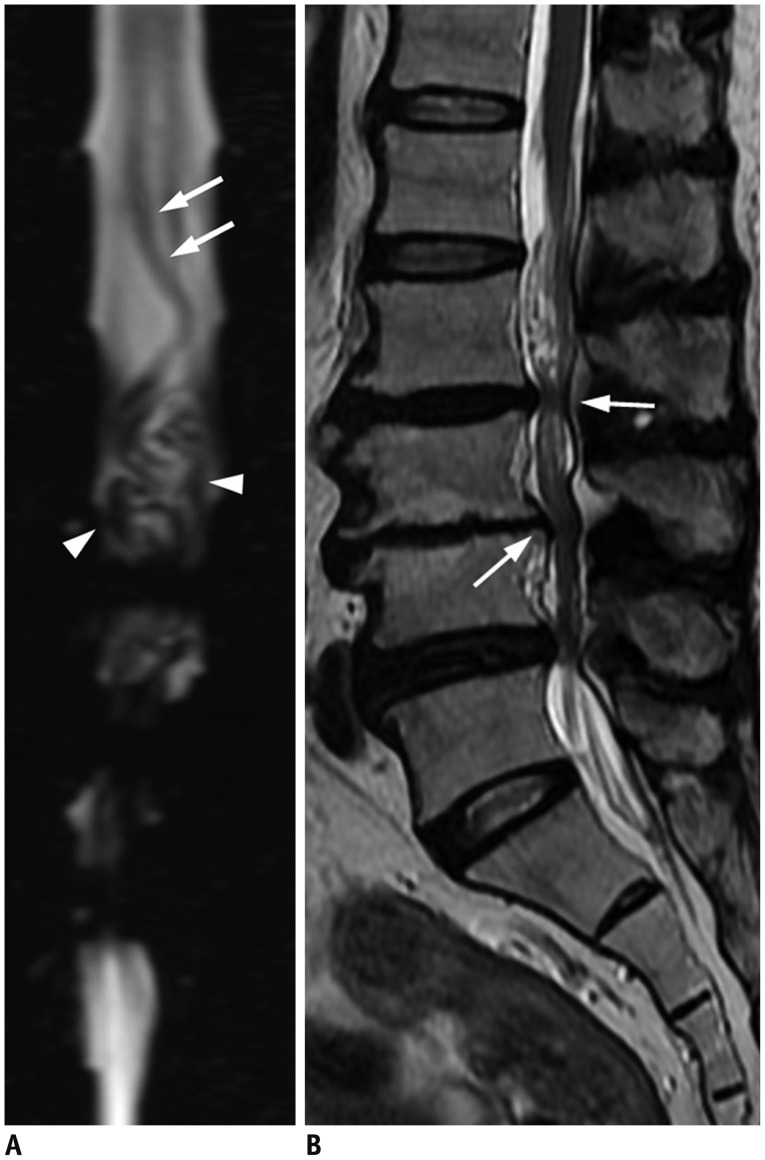
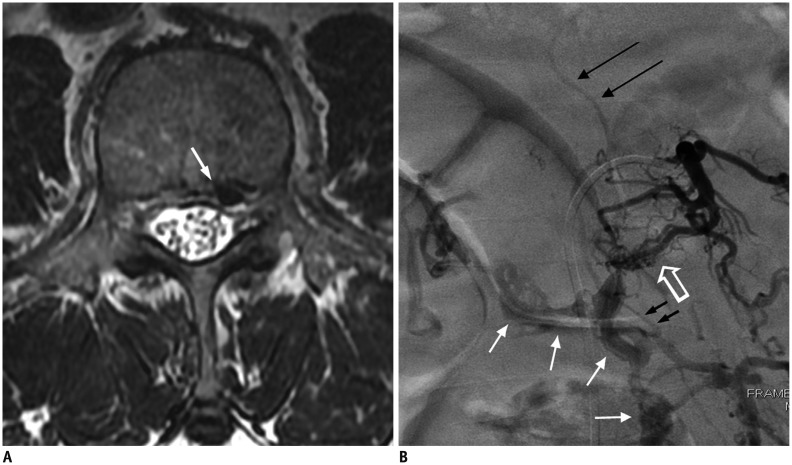
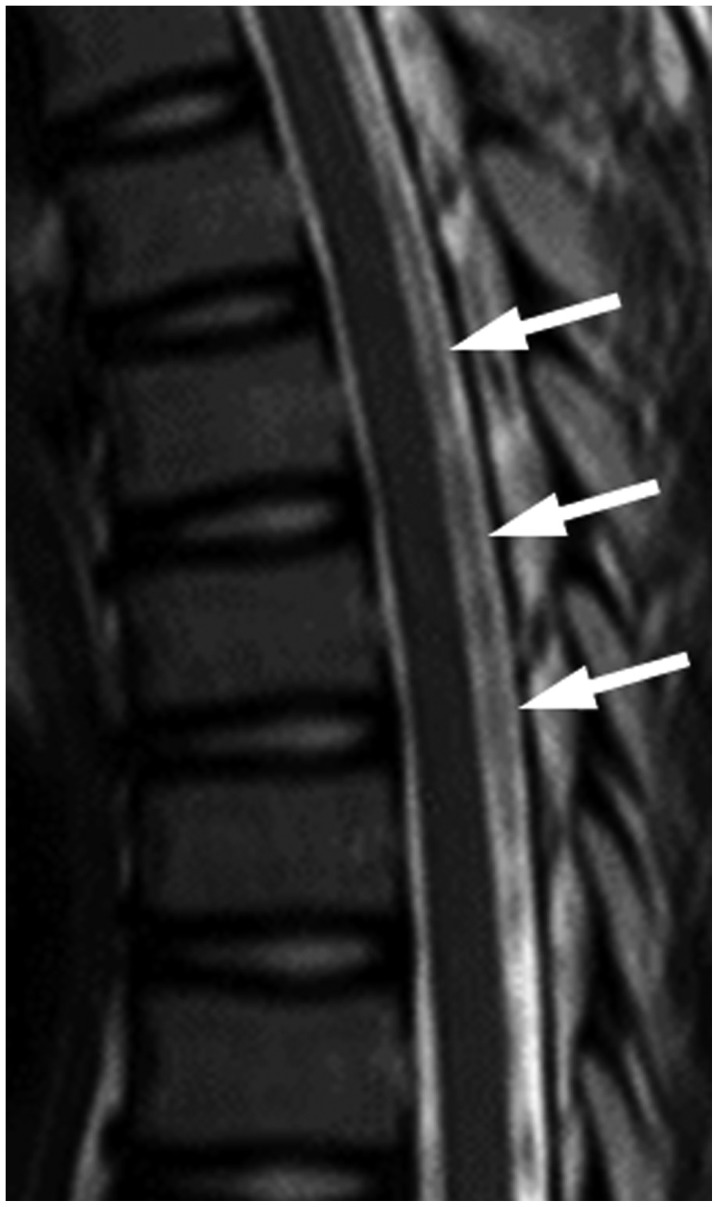
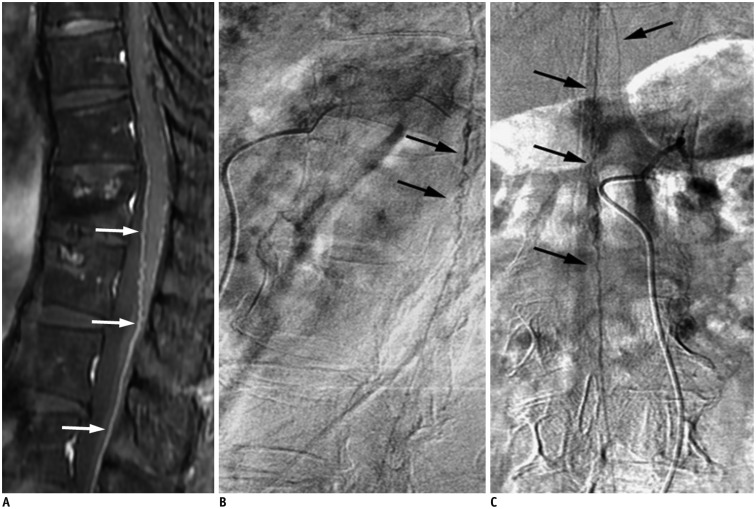
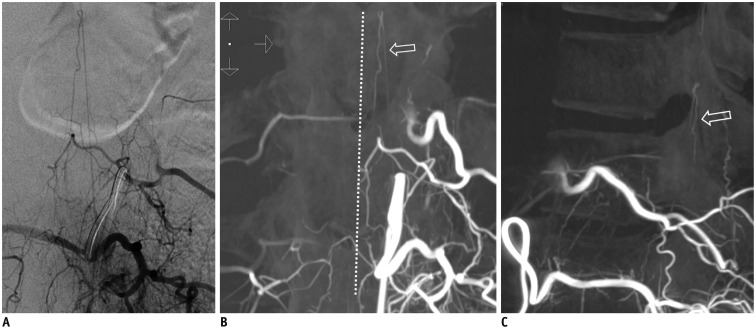
Spinal dural arteriovenous fistula (SDAVF) is the most common spinal vascular malformation, however it is still rare and underdiagnosed. Magnetic resonance imaging findings such as spinal cord edema and dilated and tortuous perimedullary veins play a pivotal role in the confirmation of the diagnosis. However, spinal angiography remains the gold standard in the diagnosis of SDAVF. Classic angiographic findings of SDAVF are early filling of radicular veins, delayed venous return, and an extensive network of dilated perimedullary venous plexus. A series of angiograms of SDAVF at different locations along the spinal column, and mimics of serpentine perimedullary venous plexus on MR images, are demonstrated. Thorough knowledge of SDAVF aids correct diagnosis and prevents irreversible complications.
Keywords: Central nervous system vascular malformations; Spinal cord diseases; Spine.
Figures




References
-
- Aminoff MJ, Logue V. The prognosis of patients with spinal vascular malformations. Brain. 1974;97:211–218. - PubMed
-
- Koch C. Spinal dural arteriovenous fistula. Curr Opin Neurol. 2006;19:69–75. - PubMed
-
- Van Dijk JM, TerBrugge KG, Willinsky RA, Farb RI, Wallace MC. Multidisciplinary management of spinal dural arteriovenous fistulas: clinical presentation and long-term follow-up in 49 patients. Stroke. 2002;33:1578–1583. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
