

Patient Care Planning Discussions for Patients at the End of Life: An Evidence-Based Analysis
- PMID: 26357528
- PMCID: PMC4561366
Patient Care Planning Discussions for Patients at the End of Life: An Evidence-Based Analysis
Abstract
Background: Ontario spends about 9% of its health budget on care for people at the end of life (EoL), most of whom die from chronic, prolonged conditions. For many people, patient care planning discussions (PCPDs) can improve the quality and reduce the cost of care.
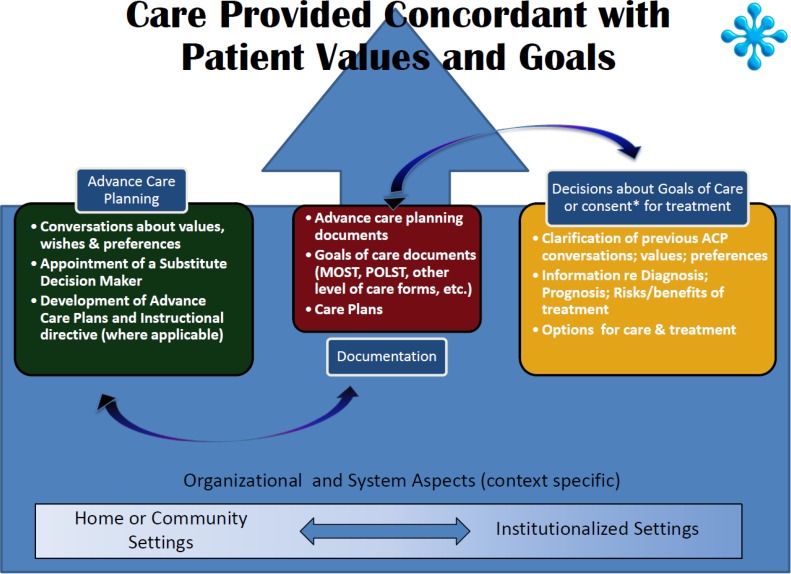
Objectives: This evidence-based analysis aimed to examine the effectiveness of PCPDs in achieving better patient-centred outcomes for people at the EoL.
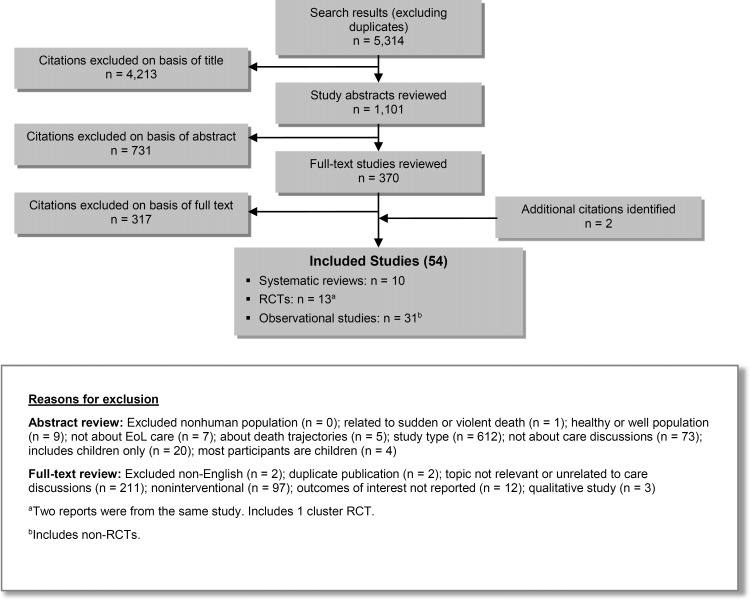
Data sources: A systematic literature search was conducted in MEDLINE, Embase, CINAHL, and EBM Reviews to identify relevant literature published between January 1, 2004, and October 9, 2013.
Review methods: Peer-reviewed reports from randomized controlled trials (RCTs) and observational studies were examined. Outcomes included quality of life (QoL), satisfaction, concordance, advance care planning (ACP), and health care use. Quality of evidence was assessed using GRADE.
Results: While the effects of PCPDs on QoL are unclear, single-provider PCPDs were associated with family members being very satisfied with EoL care (odds ratio [OR]: 5.17 [95% CI: 1.52, 17.58]), improved concordance between patients' and families' wishes (OR: 4.32, P < 0.001), fewer episodes of hospital care (mean difference [MD]: -0.21, P = 0.04), spending fewer days in hospital (MD: -1.8, P = 0.03), and receiving hospice care (OR: 5.17 [95% CI: 2.03, 13.17]). Team-based PCPDs were associated with greater patient satisfaction (standardized mean difference [SMD]: 0.39 [95% CI: 0.17, 0.60]) and fewer outpatient visits (MD: -5.20 [95% CI: -9.70, -0.70]). Overall, PCPDs were associated with more ACP and more optimal health care use.
Limitations: Most of the RCTs were unblinded, intervention was measured or described inadequately in some studies, and the term "usual care" was often undefined.
Conclusions: Patients at the EoL and their families benefited from PCPDs. Furthermore, PCPDs occurring earlier in the course of illness were associated with better outcomes than those occurring later.
Figures
References
-
- Lorenz KA, Lynn J, Morton SC, Dy SM, Shugarman LM, Wilkinson A, et al. Methodological approaches for a systematic review of end-of-life care. J Palliat Med. 2005; 8 Suppl 1: S4–11. - PubMed
-
- Statistics Canada. Table 3–6. Ten leading causes of death, by sex and geography, 2009—Ontario. [Ottawa: ]: Statistics Canada; 2012. [cited 2014 Feb. 13]. Available from: http://www.statcan.gc.ca/pub/84-215-x/2012001/tbl/t019-eng.htm.
-
- Hales S, Zimmermann C, Rodin G. The quality of dying and death. Arch Intern Med. 2008; 168(9): 912–8. - PubMed
-
- Ferrell BR. Overview of the domains of variables relevant to end-of-life care. J Palliat Med. 2005; 8 Suppl 1: S22–S29. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources