

Update on Autoimmune Hepatitis
- PMID: 26357634
- PMCID: PMC4542083
- DOI: 10.14218/JCTH.2014.00032
Update on Autoimmune Hepatitis
Abstract
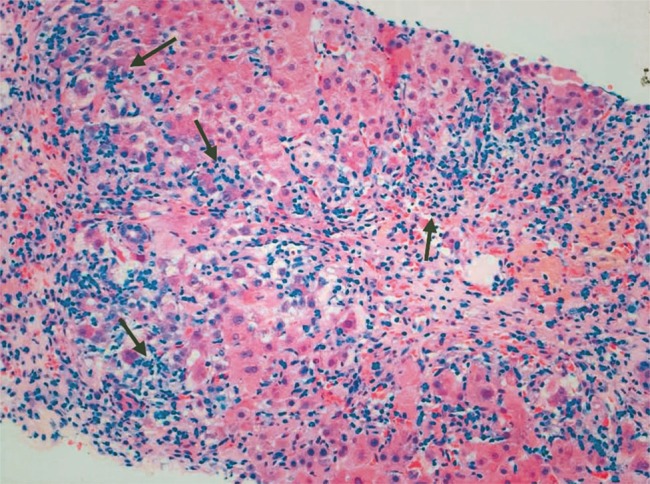
Autoimmune hepatitis (AIH), a liver disorder affecting both children and adults, is characterized by inflammatory liver histology, elevated transaminase levels, circulating nonorganspecific autoantibodies, and increased levels of immunoglobulin G, in the absence of a known etiology. Two types of AIH are recognized according to seropositivity: smooth muscle antibody and/or antinuclear antibody define AIH type 1 and antibodies to liver-kidney microsome type 1 and/or liver cytosol type 1 define AIH type 2. AIH type 1 affects both adults and children, while AIH type 2 is mainly a paediatric disease, though it does occasionally affects young adults. AIH should be considered during the diagnostic workup of any patient with increased liver enzyme levels. AIH is exquisitely responsive to immunosuppressive treatment with prednisolone with or without azathioprine, with symptom free long-term survival for the majority of patients. For those who do not respond to standard treatment, or who are difficult-to-treat, mycophenolate mofetil and, in the absence of a response, calcineurin inhibitors should be tried in addition to steroids. The pathogenesis of AIH is not fully understood, although there is mounting evidence that genetic susceptibility, molecular mimicry and impaired immunoregulatory networks contribute to the initiation and perpetuation of the autoimmune attack. Liver damage is thought to be mediated primarily by CD4 T-cells, although recent studies support the involvement of diverse populations, including Th17 cells. A deeper understanding of the pathogenesis of AIH is likely to contribute to the development of novel treatments, such as the adoptive transfer of autologous expanded antigenspecific regulatory T-cells, which ultimately aim at restoring tolerance to liver-derived antigens.
Keywords: Autoantibodies; Autoimmune hepatitis; Immunogenetics; Immunosuppresion; Regulatory T cells.
Conflict of interest statement
Figures

References
-
- Waldenstrm J. Leber Blutprotein und Nahrungseiweiss. Deutsch Z Verdau Stoffwechselkr. 1950;15:113–119. - PubMed
-
- Mackay IR, Cowling DC, Taft LI. Lupoid hepatitis. Lancet. 1956;271:1323–1326. 10.1016/S01406736(56)914830. - DOI - PubMed
-
- Cook GC, Mulligan R, Sherlock S. Controlled prospective trial of corticosteroid therapy in active chronic hepatitis. QJMed. 1971;40:159–185. 10.1093/oxfordjournals.qjmed.a067264. - DOI - PubMed
-
- Soloway RD, Summerskill WH, Baggenstoss AH, Geall MG, Gitnik GL, Elveback IR, et al. Clinical, biochemical, and histological remission of severe chronic active liver disease: a controlled study of treatments and early prognosis. Gastroenterology. 1972;63:820–833. - PubMed
-
- MurrayLyon IM, Stern RB, Williams R. Controlled trial of prednisone and azathioprine in active chronic hepatitis. Lancet. 1973;1:735–737. 10.1016/S01406736(73)921259. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials