

Attenuating the Systemic Inflammatory Response to Adult Cardiopulmonary Bypass: A Critical Review of the Evidence Base
- PMID: 26357785
- PMCID: PMC4566828
Attenuating the Systemic Inflammatory Response to Adult Cardiopulmonary Bypass: A Critical Review of the Evidence Base
Abstract
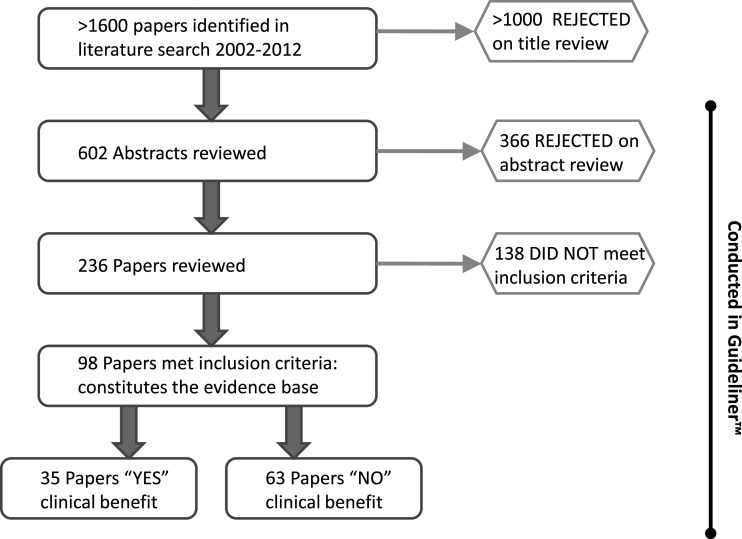
A wide range of pharmacological, surgical, and mechanical pump approaches have been studied to attenuate the systemic inflammatory response to cardiopulmonary bypass, yet no systematically based review exists to cover the scope of anti-inflammatory interventions deployed. We therefore conducted an evidence-based review to capture "self-identified" anti-inflammatory interventions among adult cardiopulmonary bypass procedures. To be included, trials had to measure at least one inflammatory mediator and one clinical outcome, specified in the "Outcomes 2010" consensus statement. Ninety-eight papers satisfied inclusion criteria and formed the basis of the review. The review identified 33 different interventions and approaches to attenuate the systemic inflammatory response. However, only a minority of papers (35 of 98 [35.7%]) demonstrated any clinical improvement to one or more of the predefined outcome measures (most frequently myocardial protection or length of intensive care unit stay). No single intervention was supported by strong level A evidence (multiple randomized controlled trials [RCTs] or meta-analysis) for clinical benefit. Interventions at level A evidence included off-pump surgery, minimized circuits, biocompatible circuit coatings, leukocyte filtration, complement C5 inhibition, preoperative aspirin, and corticosteroid prophylaxis. Interventions at level B evidence (single RCT) for minimizing inflammation included nitric oxide donors, C1 esterase inhibition, neutrophil elastase inhibition, propofol, propionyl-L-carnitine, and intensive insulin therapy. A secondary analysis revealed that suppression of at least one inflammatory marker was necessary but not sufficient to confer clinical benefit. The most effective interventions were those that targeted multiple inflammatory pathways. These observations are consistent with a "multiple hit" hypothesis, whereby clinically effective suppression of the systemic inflammatory response requires hitting multiple inflammatory targets simultaneously. Further research is warranted to evaluate if combinations of interventions that target multiple inflammatory pathways are capable of synergistically reducing inflammation and improving outcomes after cardiopulmonary bypass.
Conflict of interest statement
Dr. Likosky discloses holding a grant from the Agency for Healthcare Research and Quality (AHRQ), and has received unrestricted funds to support his research from: CASMED, Medtronic, Terumo, and Somanetics.
Figures
References
-
- Prondzinsky R, Knupfer A, Loppnow H, et al. . Surgical trauma affects the proinflammatory status after cardiac surgery to a higher degree than cardiopulmonary bypass. J Thorac Cardiovasc Surg. 2005;129:760–766. - PubMed
-
- Bittar N, Koke JR, Berkoff HA, Kahn DR.. Histochemical and structural changes in human myocardial cells after cardiopulmonary bypass. Circulation. 1975;52Suppl:I16–I25. - PubMed
-
- Chenoweth DE, Cooper SW, Hugli TE, Stewart RW, Blackstone EH, Kirklin JW.. Complement activation during cardiopulmonary bypass: Evidence for generation of C3a and C5a anaphylatoxins. N Engl J Med. 1981;304:497–503. - PubMed
-
- Brister SJ, Ofosu FA, Buchanan MR.. Thrombin generation during cardiac surgery: Is heparin the ideal anticoagulant? Thromb Haemost. 1993;70:259–262. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous