

Optimal Diagnostic Indices for Idiopathic Normal Pressure Hydrocephalus Based on the 3D Quantitative Volumetric Analysis for the Cerebral Ventricle and Subarachnoid Space
- PMID: 26359148
- PMCID: PMC7964275
- DOI: 10.3174/ajnr.A4440
Optimal Diagnostic Indices for Idiopathic Normal Pressure Hydrocephalus Based on the 3D Quantitative Volumetric Analysis for the Cerebral Ventricle and Subarachnoid Space
Abstract
Background and purpose: Despite the remarkable progress of 3D graphics technology, the Evans index has been the most popular index for ventricular enlargement. We investigated a novel reliable index for the MR imaging features specified in idiopathic normal pressure hydrocephalus, rather than the Evans index.
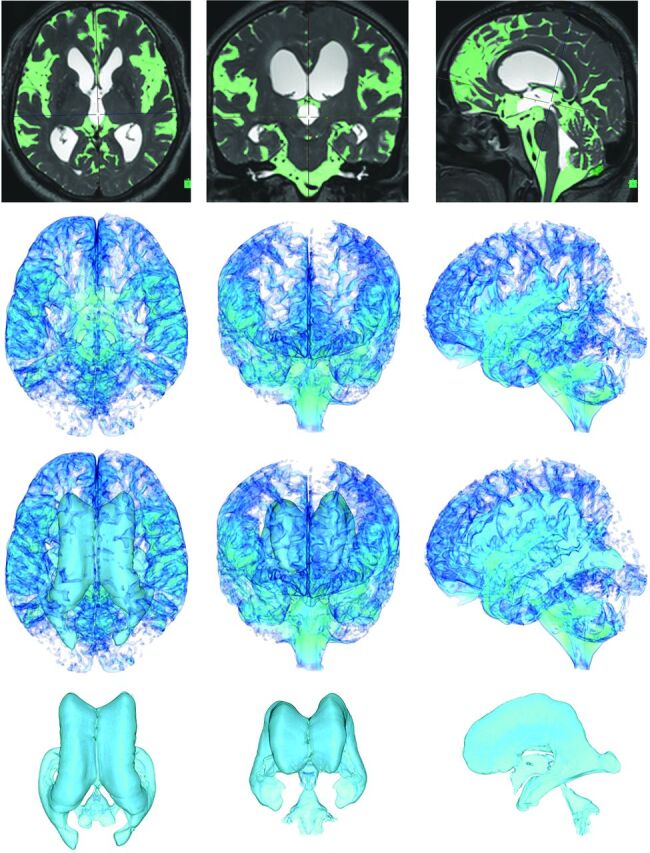
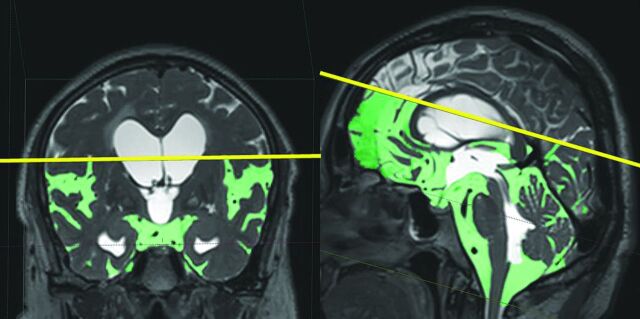
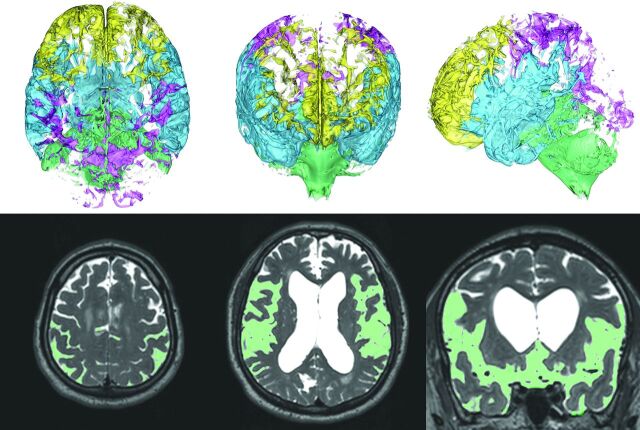
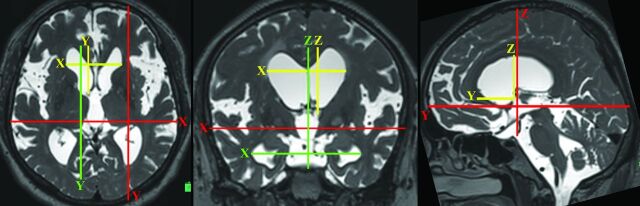
Materials and methods: The patients with suspected idiopathic normal pressure hydrocephalus on the basis of the ventriculomegaly and a triad of symptoms underwent the CSF tap test. CSF volumes were extracted from a T2-weighted 3D spin-echo sequence named "sampling perfection with application-optimized contrasts by using different flip angle evolutions (SPACE)" on 3T MR imaging and were quantified semiautomatically. Subarachnoid spaces were divided as follows: upper and lower parts and 4 compartments of frontal convexity, parietal convexity, Sylvian fissure and basal cistern, and posterior fossa. The maximum length of 3 axial directions in the bilateral ventricles and their frontal horns was measured. The "z-Evans Index" was defined as the maximum z-axial length of the frontal horns to the maximum cranial z-axial length. These parameters were evaluated for the predictive accuracy for the tap-positive groups compared with the tap-negative groups and age-adjusted odds ratios at the optimal thresholds.
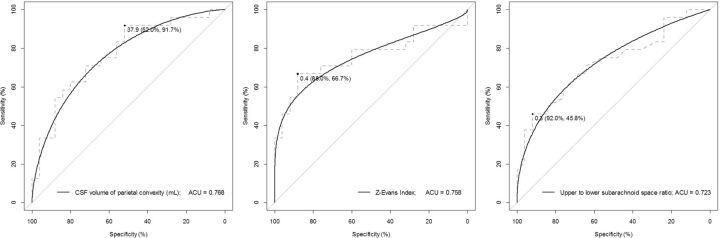
Results: In this study, 24 patients with tap-positive idiopathic normal pressure hydrocephalus, 25 patients without response to the tap test, and 23 age-matched controls were included. The frontal horns of the bilateral ventricles were expanded, with the most excessive expansion being toward the z-direction. The CSF volume of the parietal convexity had the highest area under the receiver operating characteristic curve (0.768), the z-Evans Index was the second (0.758), and the upper-to-lower subarachnoid space ratio index was the third (0.723), to discriminate the tap-test response.
Conclusions: The CSF volume of the parietal convexity of <38 mL, upper-to-lower subarachnoid space ratio of <0.33, and the z-Evans Index of >0.42 were newly proposed useful indices for the idiopathic normal pressure hydrocephalus diagnosis, an alternative to the Evans Index.
© 2015 by American Journal of Neuroradiology.
Figures
Similar articles
-
Cerebral ventriculomegaly in myotonic dystrophy type 1: normal pressure hydrocephalus-like appearances on magnetic resonance imaging.BMC Neurosci. 2021 Oct 18;22(1):62. doi: 10.1186/s12868-021-00667-8. BMC Neurosci. 2021. PMID: 34663226 Free PMC article.
-
Comparison of CSF Distribution between Idiopathic Normal Pressure Hydrocephalus and Alzheimer Disease.AJNR Am J Neuroradiol. 2016 Jul;37(7):1249-55. doi: 10.3174/ajnr.A4695. Epub 2016 Feb 25. AJNR Am J Neuroradiol. 2016. PMID: 26915568 Free PMC article.
-
Distinct volumetric features of cerebrospinal fluid distribution in idiopathic normal-pressure hydrocephalus and Alzheimer's disease.Fluids Barriers CNS. 2022 Sep 1;19(1):66. doi: 10.1186/s12987-022-00362-8. Fluids Barriers CNS. 2022. PMID: 36045420 Free PMC article.
-
Brain MRI as a predictor of CSF tap test response in patients with idiopathic normal pressure hydrocephalus.J Neurol. 2010 Oct;257(10):1675-81. doi: 10.1007/s00415-010-5602-8. Epub 2010 May 29. J Neurol. 2010. PMID: 20512347 Review.
-
Neuroimaging of Adult Hydrocephalus.Neurosurg Clin N Am. 2025 Apr;36(2):183-197. doi: 10.1016/j.nec.2024.11.007. Epub 2025 Jan 24. Neurosurg Clin N Am. 2025. PMID: 40054972 Review.
Cited by
-
Imaging Markers for Normal Pressure Hydrocephalus: An Overview.Biomedicines. 2023 Apr 24;11(5):1265. doi: 10.3390/biomedicines11051265. Biomedicines. 2023. PMID: 37238936 Free PMC article. Review.
-
Automatic assessment of disproportionately enlarged subarachnoid-space hydrocephalus from 3D MRI using two deep learning models.Front Aging Neurosci. 2024 Mar 15;16:1362637. doi: 10.3389/fnagi.2024.1362637. eCollection 2024. Front Aging Neurosci. 2024. PMID: 38560023 Free PMC article.
-
MRI markers of idiopathic normal pressure hydrocephalus in a population study with 791 participants: Exploring reference values and associations.Neuroradiol J. 2025 Aug;38(4):475-487. doi: 10.1177/19714009241303132. Epub 2024 Dec 9. Neuroradiol J. 2025. PMID: 39648970 Free PMC article.
-
Splenial angle on axial T1 and fluid-attenuated inversion-recovery MRI images and idiopathic normal pressure hydrocephalus.Br J Radiol. 2025 Jun 1;98(1170):938-946. doi: 10.1093/bjr/tqaf058. Br J Radiol. 2025. PMID: 40088925 Free PMC article.
-
Cerebral ventriculomegaly in myotonic dystrophy type 1: normal pressure hydrocephalus-like appearances on magnetic resonance imaging.BMC Neurosci. 2021 Oct 18;22(1):62. doi: 10.1186/s12868-021-00667-8. BMC Neurosci. 2021. PMID: 34663226 Free PMC article.
References
-
- Marmarou A, Bergsneider M, Relkin N, et al. . Development of guidelines for idiopathic normal-pressure hydrocephalus: introduction. Neurosurgery 2005;57:S1–3; discussion ii–v - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous