

Split-bolus MR urography: synchronous visualization of obstructing vessels and collecting system in children
- PMID: 26359874
- PMCID: PMC4622399
- DOI: 10.5152/dir.2015.15068
Split-bolus MR urography: synchronous visualization of obstructing vessels and collecting system in children
Abstract
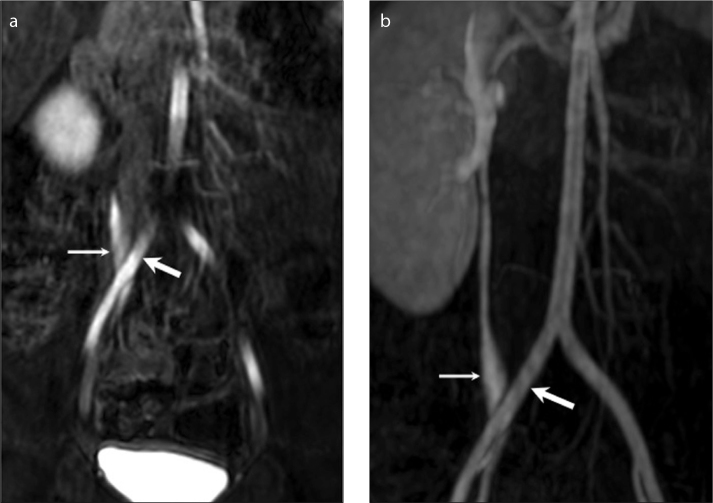
Several vascular abnormalities related with urinary system such as crossing accessory renal vessels, retroiliac ureters, retrocaval ureters, posterior nutcracker syndrome, and ovarian vein syndrome may be responsible for urinary collecting system obstruction. Split-bolus magnetic resonance urography (MRU) using contrast material as two separate bolus injections provides superior demonstration of the collecting system and obstructing vascular anomalies simultaneously and enables accurate preoperative radiologic diagnosis. In this pictorial review we aimed to outline the split-bolus MRU technique in children, list the coexisting congenital collecting system and vascular abnormalities, and exhibit the split-bolus MRU appearances of concurrent urinary collecting system and vascular abnormalities.
Figures







References
-
- Levendecker JR, Barnes CE, Zagoria RJ. MR urography: techniques and clinical applications. Radiographics. 2008;28:23–46. http://dx.doi.org/10.1148/rg.281075077. - DOI - PubMed
-
- Battal B, Kocaoglu M, Akgun V, Aydur E, Dayanc M, Ilica T. Feasibility of MR urography in patients with urinary diversion. J Med Imaging Radiat Oncol. 2011;55:542–550. http://dx.doi.org/10.1111/j.1754-9485.2011.02318.x. - DOI - PubMed
-
- Koçyiğit A, Yüksel S, Bayram R, Yılmaz İ, Karabulut N. Efficacy of magnetic resonance urography in detecting renal scars in children with vesicoureteral reflux. Pediatr Nephrol. 2014;29:1215–1220. http://dx.doi.org/10.1007/s00467-014-2766-y. - DOI - PubMed
-
- Kocyigit A, Serinken M, Ceven Z, et al. A strategy to optimize CT use in children with mild blunt head trauma utilizing clinical risk stratification; could we improve CT use in children with mild head injury? Clin Imaging. 2014;38:236–240. http://dx.doi.org/10.1016/j.clinimag.2013.12.004. - DOI - PubMed
-
- Kocaoglu M, Bulakbasi N, Ilica AT, Gok F, Tayfun C, Somuncu I. Intravenous contrast-enhanced dynamic MR urography: diagnosis of vesicoureteral reflux during bladder filling with time-signal intensity curves. J Magn Reson Imaging. 2006;24:349–355. http://dx.doi.org/10.1002/jmri.20637. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
