

Persistent Hypogonadotropic Hypogonadism in Men After Severe Traumatic Brain Injury: Temporal Hormone Profiles and Outcome Prediction
- PMID: 26360007
- PMCID: PMC4786474
- DOI: 10.1097/HTR.0000000000000188
Persistent Hypogonadotropic Hypogonadism in Men After Severe Traumatic Brain Injury: Temporal Hormone Profiles and Outcome Prediction
Abstract
Objective: To (1) examine relationships between persistent hypogonadotropic hypogonadism (PHH) and long-term outcomes after severe traumatic brain injury (TBI); and (2) determine whether subacute testosterone levels can predict PHH.
Setting: Level 1 trauma center at a university hospital.
Participants: Consecutive sample of men with severe TBI between 2004 and 2009.
Design: Prospective cohort study.
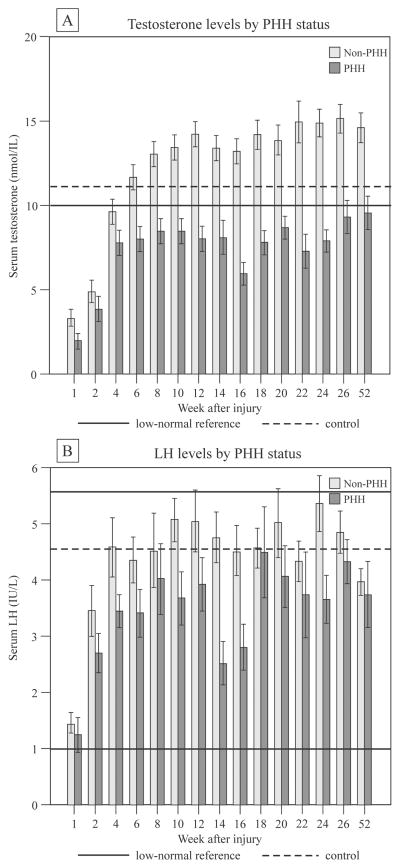
Main measures: Post-TBI blood samples were collected during week 1, every 2 weeks until 26 weeks, and at 52 weeks. Serum hormone levels were measured, and individuals were designated as having PHH if 50% or more of samples met criteria for hypogonadotropic hypogonadism. At 6 and 12 months postinjury, we assessed global outcome, disability, functional cognition, depression, and quality of life.
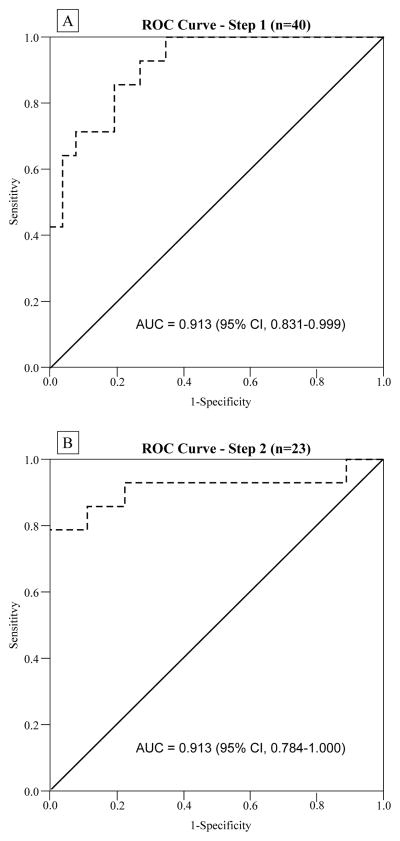
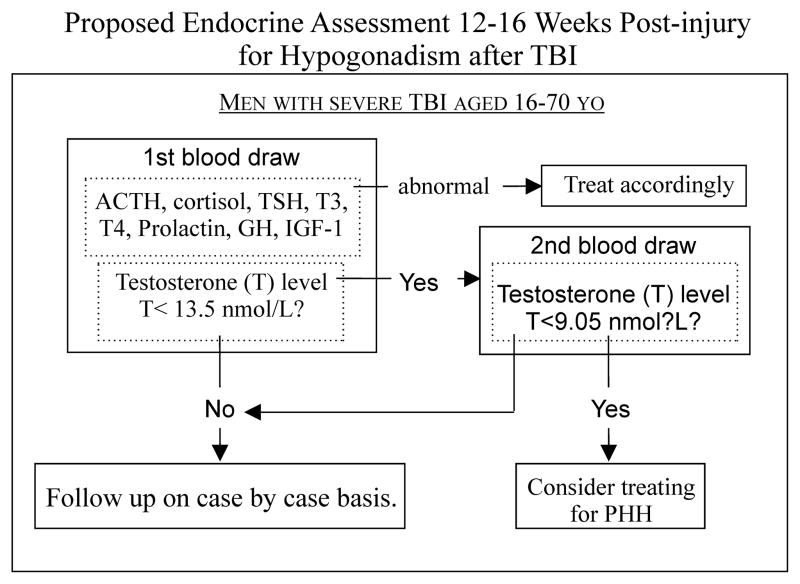
Results: We recruited 78 men; median (interquartile range) age was 28.5 (22-42) years. Thirty-four patients (44%) had PHH during the first year postinjury. Multivariable regression, controlling for age, demonstrated PHH status predicted worse global outcome scores, more disability, and reduced functional cognition at 6 and 12 months post-TBI. Two-step testosterone screening for PHH at 12 to 16 weeks postinjury yielded a sensitivity of 79% and specificity of 100%.
Conclusion: PHH status in men predicts poor outcome after severe TBI, and PHH can accurately be predicted at 12 to 16 weeks.
Conflict of interest statement
Figures
Similar articles
-
Persistent hypogonadism influences estradiol synthesis, cognition and outcome in males after severe TBI.Brain Inj. 2012;26(10):1226-42. doi: 10.3109/02699052.2012.667594. Epub 2012 May 9. Brain Inj. 2012. PMID: 22571223
-
Anti-Pituitary and Anti-Hypothalamus Autoantibody Associations with Inflammation and Persistent Hypogonadotropic Hypogonadism in Men with Traumatic Brain Injury.J Neurotrauma. 2020 Jul 15;37(14):1609-1626. doi: 10.1089/neu.2019.6780. Epub 2020 Apr 13. J Neurotrauma. 2020. PMID: 32111134 Free PMC article.
-
Functional Outcomes Over the First Year After Moderate to Severe Traumatic Brain Injury in the Prospective, Longitudinal TRACK-TBI Study.JAMA Neurol. 2021 Aug 1;78(8):982-992. doi: 10.1001/jamaneurol.2021.2043. JAMA Neurol. 2021. PMID: 34228047 Free PMC article.
-
Chronic impact of traumatic brain injury on outcome and quality of life: a narrative review.Crit Care. 2016 Jun 21;20(1):148. doi: 10.1186/s13054-016-1318-1. Crit Care. 2016. PMID: 27323708 Free PMC article. Review.
-
Hypogonadism after traumatic brain injury.Arq Bras Endocrinol Metabol. 2009 Nov;53(8):908-14. doi: 10.1590/s0004-27302009000800003. Arq Bras Endocrinol Metabol. 2009. PMID: 20126842 Review.
Cited by
-
Endocrine dysfunction post-traumatic brain injury: challenges and therapeutic approaches.Acta Neurol Belg. 2025 Jun;125(3):649-660. doi: 10.1007/s13760-025-02755-6. Epub 2025 Mar 7. Acta Neurol Belg. 2025. PMID: 40053294 Review.
-
Beyond Binary: Influence of Sex and Gender on Outcome after Traumatic Brain Injury.J Neurotrauma. 2020 Dec 1;37(23):2454-2459. doi: 10.1089/neu.2020.7230. Epub 2020 Sep 2. J Neurotrauma. 2020. PMID: 32808570 Free PMC article. Review.
-
Neurobiological Mechanisms Underlying Psychological Dysfunction After Brain Injuries.Cells. 2025 Jan 8;14(2):74. doi: 10.3390/cells14020074. Cells. 2025. PMID: 39851502 Free PMC article. Review.
-
Rehabilomics: A state-of-the-art review of framework, application, and future considerations.Front Neurol. 2023 Mar 8;14:1103349. doi: 10.3389/fneur.2023.1103349. eCollection 2023. Front Neurol. 2023. PMID: 36970504 Free PMC article. Review.
-
Multifetal gestations after traumatic brain injury: a nationwide register-based cohort study in Finland.BMC Pregnancy Childbirth. 2023 Apr 4;23(1):228. doi: 10.1186/s12884-023-05539-z. BMC Pregnancy Childbirth. 2023. PMID: 37016336 Free PMC article.
References
-
- Centers for Disease Control and Prevention, National Center for Injury Prevention and Control Website. Traumatic Brain Injury in the United States: Fact Sheet.
-
- Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Rates of TBI-related Emergency Department Visits, Hospitalizations, and Deaths by Sex — United States, 2001–2010.
-
- Zaloshnja E, Miller T, Langlois JA, Selassie AW. Prevalence of long-term disability from traumatic brain injury in the civilian population of the United States, 2005. J Head Trauma Rehabil. 2008;23(6):394–400. - PubMed
-
- Hohl A, Ronsoni MF, van de Sande-Lee S, et al. Androgens, Male Hypogonadism and Traumatic Brain Injury. Open J Endocr Metab Dis. 2014;04(01):13–23.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
