

Polio revisited: reviving knowledge and skills to meet the challenge of resurgence
- PMID: 26362170
- PMCID: PMC4619376
- DOI: 10.1007/s11832-015-0678-4
Polio revisited: reviving knowledge and skills to meet the challenge of resurgence
Abstract
Purpose: To date, polio has not been eradicated and there appears to be a resurgence of the disease. Hence, there is a need to revive decision-making skills to treat the effects of polio.
Methods: Here, we outline the aspects of treatment of paralysis following polio based on the literature and personal experience of the authors. The surgical treatment of the lower and upper extremities and the spine have been reviewed. The scope of bracing of the lower limb has been defined.
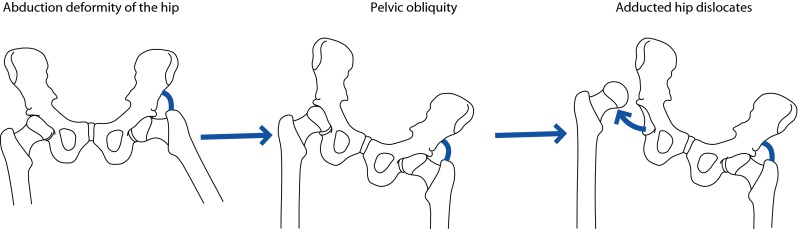
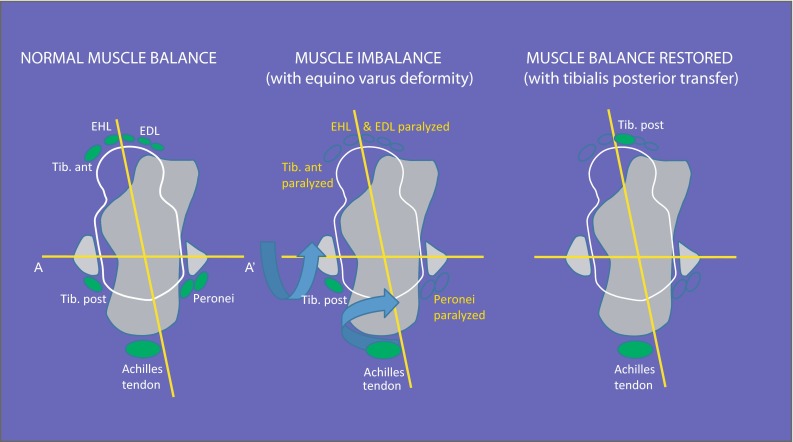
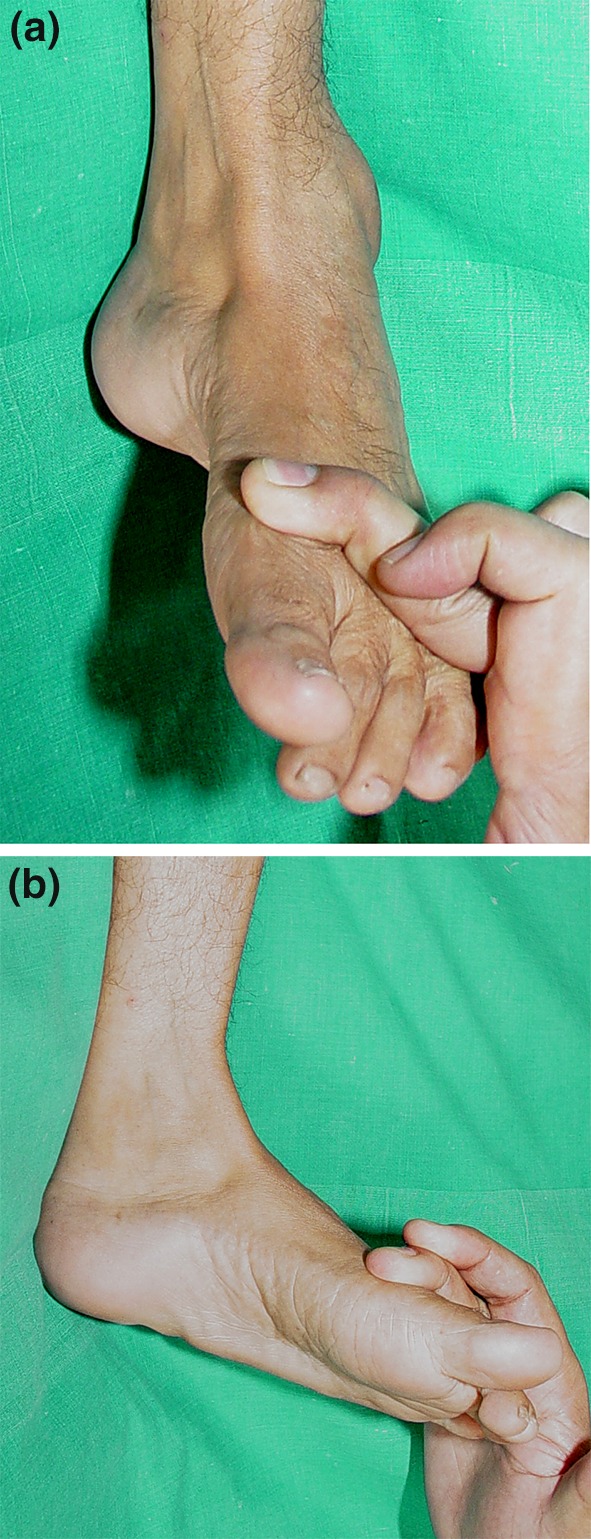
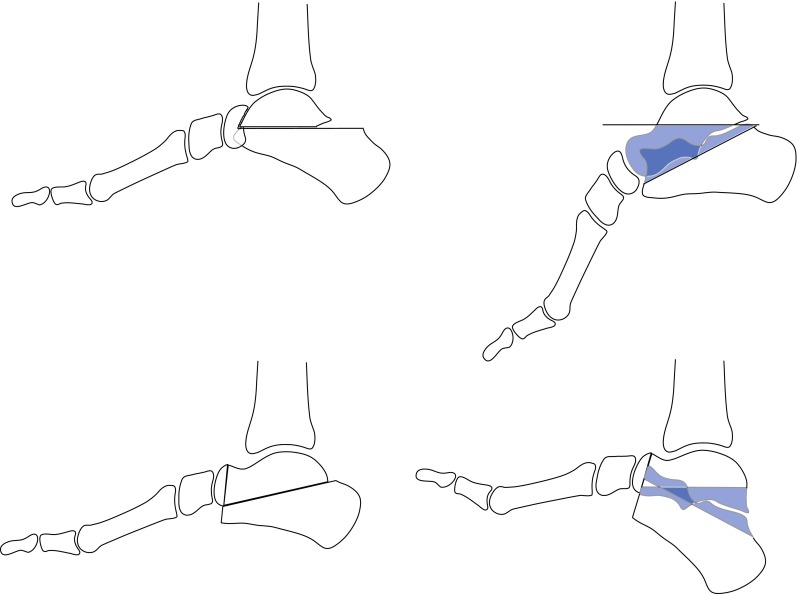
Results: The effects of polio can be mitigated by judicious correction of deformities, restoration of muscle balance, stabilising unstable joints and compensating for limb length inequality.
Conclusions: As polio has not been eradicated and there is a risk of resurgence of the disease, paediatric orthopaedic surgeons need to be prepared to deal with fresh cases of polio. Revival of old techniques for managing the effects of paralysis following polio is needed.
Keywords: Bracing; Paralytic deformity; Poliomyelitis; Resurgence; Surgical decision-making.
Figures








Similar articles
-
The Uneventful Use of Modern-Day Anesthetic Drugs in Post-polio Paralytic Patients: A Report of Three Cases.Cureus. 2023 Aug 22;15(8):e43913. doi: 10.7759/cureus.43913. eCollection 2023 Aug. Cureus. 2023. PMID: 37746429 Free PMC article.
-
Vaccine-associated paralytic poliomyelitis and other diseases with acute flaccid paralysis syndrome in Belarus.Cent Eur J Public Health. 2003 Dec;11(4):213-8. Cent Eur J Public Health. 2003. PMID: 14768785
-
Defining Polio: Closing the Gap in Global Surveillance.Ann Glob Health. 2015 May-Jun;81(3):386-95. doi: 10.1016/j.aogh.2015.06.007. Ann Glob Health. 2015. PMID: 26615073
-
The polio endgame.Hum Vaccin Immunother. 2014;10(7):2106-8. doi: 10.4161/21645515.2014.981115. Hum Vaccin Immunother. 2014. PMID: 25608050 Free PMC article. Review.
-
Poliomyelitis.Handb Clin Neurol. 2018;159:337-344. doi: 10.1016/B978-0-444-63916-5.00021-5. Handb Clin Neurol. 2018. PMID: 30482325 Review.
Cited by
-
ACL Reconstruction using Achilles Allograft in a Case of Genu Recurvatum with Supracondylar Osteotomy.J Orthop Case Rep. 2024 Apr;14(4):58-62. doi: 10.13107/jocr.2024.v14.i04.4358. J Orthop Case Rep. 2024. PMID: 38681917 Free PMC article.
-
The Uneventful Use of Modern-Day Anesthetic Drugs in Post-polio Paralytic Patients: A Report of Three Cases.Cureus. 2023 Aug 22;15(8):e43913. doi: 10.7759/cureus.43913. eCollection 2023 Aug. Cureus. 2023. PMID: 37746429 Free PMC article.
-
Arthroscopic Ankle Fusion in the Post-Polio Paralytic Foot.Arthrosc Tech. 2025 Apr 26;14(6):103547. doi: 10.1016/j.eats.2025.103547. eCollection 2025 Jun. Arthrosc Tech. 2025. PMID: 40656690 Free PMC article.
-
Lower Extremity Nerve Transfers in Acute Flaccid Myelitis Patients: A Case Series.Plast Reconstr Surg Glob Open. 2021 Jul 20;9(7):e3699. doi: 10.1097/GOX.0000000000003699. eCollection 2021 Jul. Plast Reconstr Surg Glob Open. 2021. PMID: 34422521 Free PMC article.
-
Letter to the Editor: Art in Science: Jusepe de Ribera's Puzzle in The Clubfoot.Clin Orthop Relat Res. 2018 Nov;476(11):2290. doi: 10.1097/CORR.0000000000000482. Clin Orthop Relat Res. 2018. PMID: 30188346 Free PMC article. No abstract available.
References
-
- World Health Organization Country Office Tajikistan, WHO Regional Office for Europe, European Centre for Disease Prevention and Control (2010) Outbreak of poliomyelitis in Tajikistan in 2010: risk for importation and impact on polio surveillance in Europe? Euro Surveill 15(17) - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
