

The prevalence and significance of abnormal vital signs prior to in-hospital cardiac arrest
- PMID: 26362486
- PMCID: PMC4715919
- DOI: 10.1016/j.resuscitation.2015.08.016
The prevalence and significance of abnormal vital signs prior to in-hospital cardiac arrest
Abstract
Background: Patients suffering in-hospital cardiac arrest often show signs of physiological deterioration before the event. The purpose of this study was to determine the prevalence of abnormal vital signs 1-4h before cardiac arrest, and to evaluate the association between these vital sign abnormalities and in-hospital mortality.
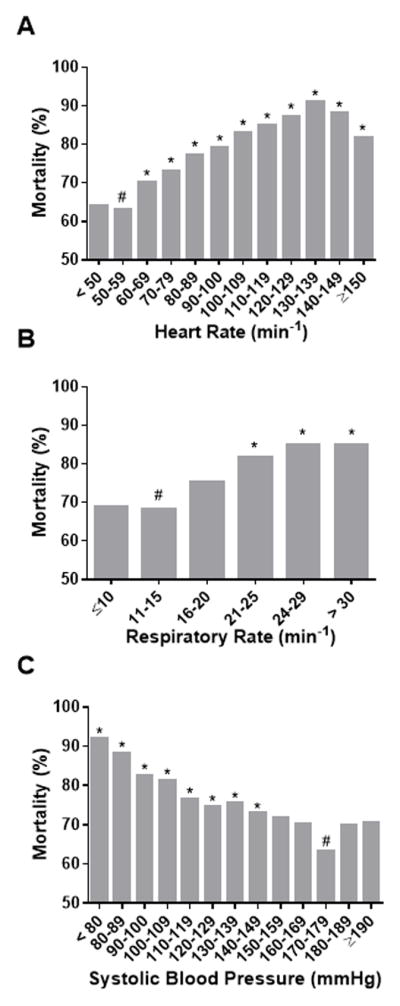
Methods: We included adults from the Get With the Guidelines(®)- Resuscitation registry with an in-hospital cardiac arrest. We used two a priori definitions for vital signs: abnormal (heart rate (HR) ≤ 60 or ≥ 100 min(-1), respiratory rate (RR) ≤ 10 or >20 min(-1) and systolic blood pressure (SBP) ≤ 90 mm Hg) and severely abnormal (HR ≤ 50 or ≥ 130 min(-1), RR ≤ 8 or ≥ 30 min(-1) and SBP ≤ 80 mm Hg). We evaluated the association between the number of abnormal vital signs and in-hospital mortality using a multivariable logistic regression model.
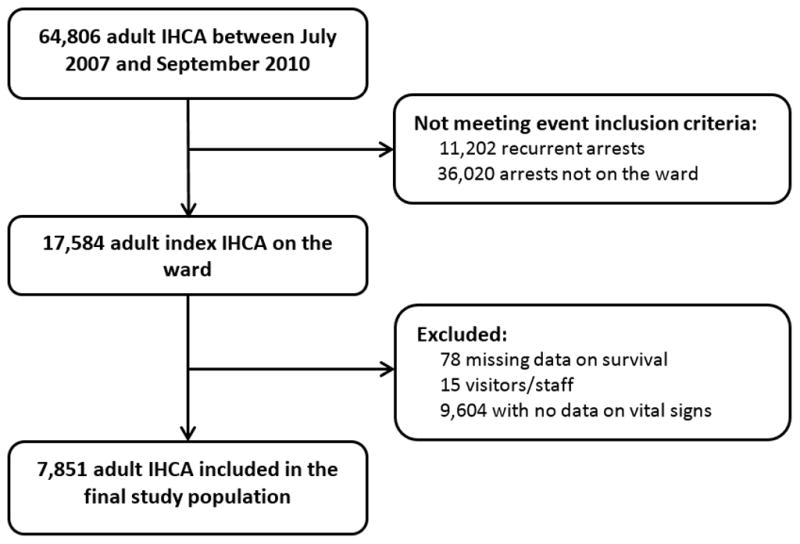
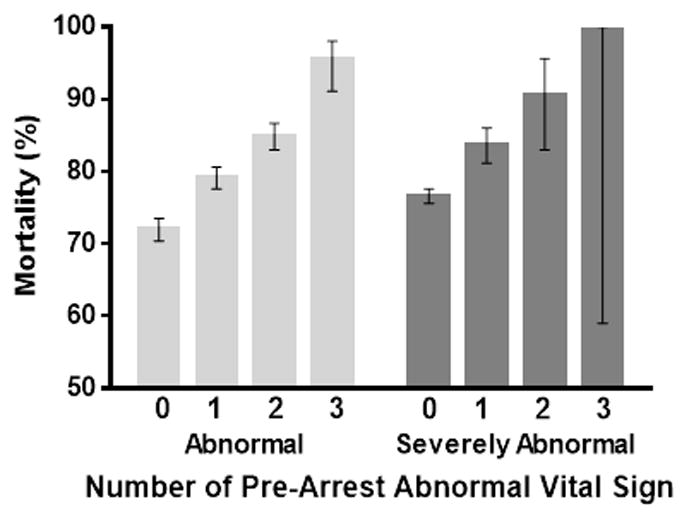
Results: 7851 patients were included. Individual vital signs were associated with in-hospital mortality. The majority of patients (59.4%) had at least one abnormal vital sign 1-4h before the arrest and 13.4% had at least one severely abnormal sign. We found a step-wise increase in mortality with increasing number of abnormal vital signs within the abnormal (odds ratio (OR) 1.53 (CI: 1.42-1.64) and severely abnormal groups (OR 1.62 (CI: 1.38-1.90)). This remained in multivariable analysis (abnormal: OR 1.38 (CI: 1.28-1.48), and severely abnormal: OR 1.40 (CI: 1.18-1.65)).
Conclusion: Abnormal vital signs are prevalent 1-4h before in-hospital cardiac arrest on hospital wards. In-hospital mortality increases with increasing number of pre-arrest abnormal vital signs as well as increased severity of vital sign derangements.
Keywords: Blood pressure; Cardiopulmonary resuscitation; Heart arrest; Heart rate; Mortality; Respiration.
Copyright © 2015 Elsevier Ireland Ltd. All rights reserved.
Conflict of interest statement
None declared
Figures
Comment in
-
Vital signs: Vital for surviving in-hospital cardiac arrest?Resuscitation. 2016 Jan;98:A3-4. doi: 10.1016/j.resuscitation.2015.10.010. Epub 2015 Oct 24. Resuscitation. 2016. PMID: 26597106 No abstract available.
References
-
- Brennan TA, Leape LL, Laird NM, et al. Incidence of adverse events and negligence in hospitalized patients. Results of the Harvard Medical Practice Study I. The New England journal of medicine. 1991;324:370–6. - PubMed
-
- Kohn LTCJ, Donaldson MS, editors. To err is human: building a safer health system. Washington, DC: national academy press; 2000. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
