

Effects of Cardiac Resynchronization Therapy on Cardiac Remodeling and Contractile Function: Results From Resynchronization Reverses Remodeling in Systolic Left Ventricular Dysfunction (REVERSE)
- PMID: 26363005
- PMCID: PMC4599493
- DOI: 10.1161/JAHA.115.002054
Effects of Cardiac Resynchronization Therapy on Cardiac Remodeling and Contractile Function: Results From Resynchronization Reverses Remodeling in Systolic Left Ventricular Dysfunction (REVERSE)
Abstract
Background: Cardiac resynchronization therapy results in improved ejection fraction in patients with heart failure. We sought to determine whether these effects were mediated by changes in contractility, afterload, or volumes.
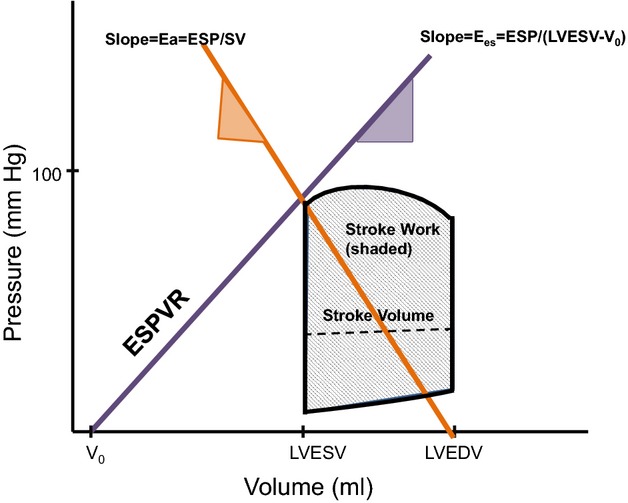
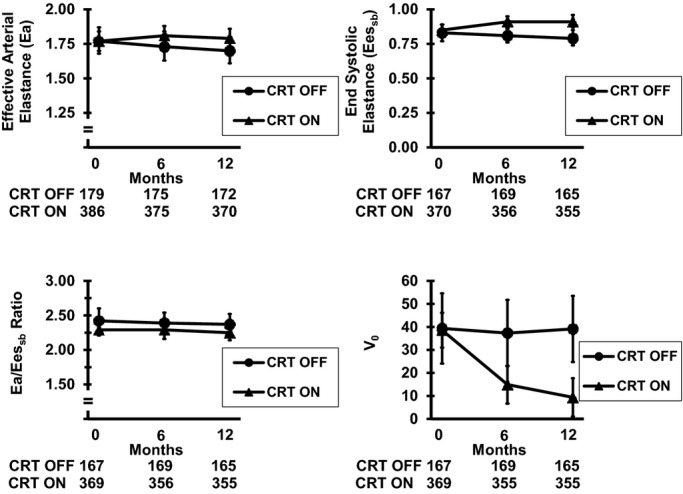
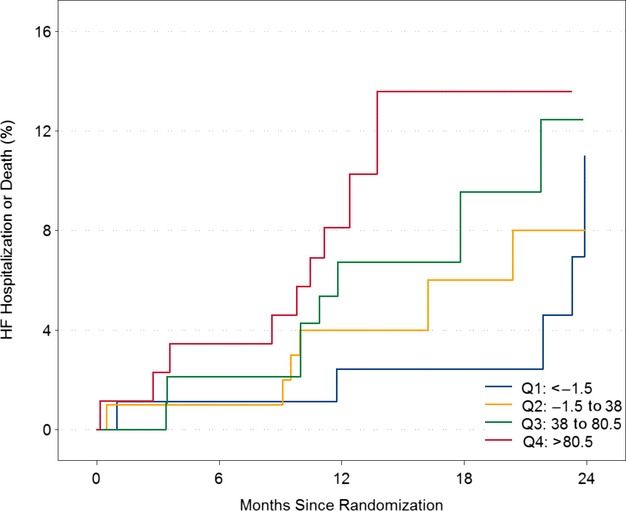
Methods and results: In 610 patients with New York Heart Association class I/II heart failure from the Resynchronization Reverses Remodeling in Systolic Left Ventricular Dysfunction (REVERSE) study, we performed detailed quantitative echocardiography assessment prior to and following cardiac resynchronization therapy. We derived measures of contractility (the slope [end-systolic elastance] and the volume intercept of the end-systolic pressure-volume relationship, stroke work, and preload recruitable stroke work), measures of arterial load and ventricular-arterial coupling, and measures of chamber size (volume intercept, end-systolic and end-diastolic volumes). At 6 and 12 months, cardiac resynchronization therapy was associated with a reduction in the volume intercept and end-systolic and end-diastolic volumes (P<0.01). There were no consistent effects on end-systolic elastance, stroke work, preload recruitable stroke work, or ventricular-arterial coupling. In the active cardiac resynchronization therapy population, baseline measures of arterial load were associated with the clinical composite score (odds ratio 1.30, 95% CI 1.04 to 1.63, P=0.02). The volume intercept was associated with mortality (hazard ratio 1.90, 95% CI 1.01 to 3.59, P=0.047) and more modestly with the combined end point of mortality or heart failure hospitalization (hazard ratio 1.48, 95% CI 0.8 to 2.25, P=0.06). In contrast, end-systolic elastance, stroke work, preload recruitable stroke work, and ventricular-arterial coupling were not associated with any outcomes.
Conclusion: In patients with NYHA Class I/II heart failure, cardiac resynchronization therapy exerts favorable changes in left ventricular end-systolic and end-diastolic volumes and the volume intercept. The volume intercept may be useful to gain insight into prognosis in heart failure.
Clinical trial registration: URL: https://www.clinicaltrials.gov/. Unique identifier: NCT00271154.
Keywords: cardiac resynchronization; echocardiography; heart failure.
© 2015 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
Similar articles
-
Left Ventricular Reverse Remodeling With Biventricular Versus Right Ventricular Pacing in Patients With Atrioventricular Block and Heart Failure in the BLOCK HF Trial.Circ Heart Fail. 2015 May;8(3):510-8. doi: 10.1161/CIRCHEARTFAILURE.114.001626. Epub 2015 Feb 19. Circ Heart Fail. 2015. PMID: 25697851 Clinical Trial.
-
Long-term impact of cardiac resynchronization therapy in mild heart failure: 5-year results from the REsynchronization reVErses Remodeling in Systolic left vEntricular dysfunction (REVERSE) study.Eur Heart J. 2013 Sep;34(33):2592-9. doi: 10.1093/eurheartj/eht160. Epub 2013 May 2. Eur Heart J. 2013. PMID: 23641006 Clinical Trial.
-
Impact of ejection fraction on the clinical response to cardiac resynchronization therapy in mild heart failure.Circ Heart Fail. 2013 Nov;6(6):1180-9. doi: 10.1161/CIRCHEARTFAILURE.113.000326. Epub 2013 Sep 6. Circ Heart Fail. 2013. PMID: 24014828 Clinical Trial.
-
Right ventricular lead location and outcomes among patients with cardiac resynchronization therapy: A meta-analysis.Prog Cardiovasc Dis. 2021 May-Jun;66:53-60. doi: 10.1016/j.pcad.2021.04.002. Epub 2021 Apr 20. Prog Cardiovasc Dis. 2021. PMID: 33864874 Free PMC article.
-
[Cardiac resynchronization therapy in terminal heart failure: current status and prospects].Herz. 2001 Feb;26(1):84-8. doi: 10.1007/pl00002010. Herz. 2001. PMID: 11258115 Review. German.
Cited by
-
What Are the Expectations for Cardiac Resynchronization Therapy? A Validation of Two Response Definitions.J Clin Med. 2021 Feb 1;10(3):514. doi: 10.3390/jcm10030514. J Clin Med. 2021. PMID: 33535633 Free PMC article.
-
Expanding benefits from cardiac resynchronization therapy to exercise-induced left bundle branch block in advanced heart failure.ESC Heart Fail. 2020 Feb;7(1):329-333. doi: 10.1002/ehf2.12580. Epub 2020 Jan 10. ESC Heart Fail. 2020. PMID: 31923352 Free PMC article.
-
Outcomes of Spironolactone Withdrawal in Dilated Cardiomyopathy With Improved Ejection Fraction.Front Cardiovasc Med. 2021 Sep 16;8:725399. doi: 10.3389/fcvm.2021.725399. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 34604354 Free PMC article.
-
Effect of Atrioventricular Dyssynchrony on Impella Hemodynamics: Mechanism and Its Clinical Implications.Cardiol Res. 2021 Aug;12(4):219-224. doi: 10.14740/cr1287. Epub 2021 Jul 9. Cardiol Res. 2021. PMID: 34349862 Free PMC article. Review.
-
Acute contractile recovery extent during biventricular pacing is not associated with follow-up in patients undergoing resynchronization.Int J Cardiol Heart Vasc. 2016 Apr 1;11:66-73. doi: 10.1016/j.ijcha.2016.03.012. eCollection 2016 Jun. Int J Cardiol Heart Vasc. 2016. PMID: 28616528 Free PMC article.
References
-
- Moss AJ, Hall WJ, Cannom DS, Klein H, Brown MW, Daubert JP, Estes NA, III, Foster E, Greenberg H, Higgins SL, Pfeffer MA, Solomon SD, Wilber D, Zareba W MADIT-CRT Trial Investigators. Cardiac-resynchronization therapy for the prevention of heart-failure events. N Engl J Med. 2009;361:1329–1338. - PubMed
-
- St John Sutton M, Ghio S, Plappert T, Tavazzi L, Scelsi L, Daubert C, Abraham WT, Gold MR, Hassager C, Herre JM, Linde C REsynchronization reVErses Remodeling in Systolic left vEntricular dysfunction (REVERSE) Study Group. Cardiac resynchronization induces major structural and functional reverse remodeling in patients with New York Heart Association class I/II heart failure. Circulation. 2009;120:1858–1865. - PubMed
-
- Linde C, Abraham WT, Gold MR, Daubert C REVERSE Study Group. Cardiac resynchronization therapy in asymptomatic or mildly symptomatic heart failure patients in relation to etiology: results from the REVERSE (REsynchronization reVErses Remodeling in Systolic Left vEntricular Dysfunction) study. J Am Coll Cardiol. 2010;56:1826–1831. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
