

Multiple Endocrine Neoplasia: Genetics and Clinical Management
- PMID: 26363542
- PMCID: PMC4571281
- DOI: 10.1016/j.soc.2015.06.008
Multiple Endocrine Neoplasia: Genetics and Clinical Management
Abstract
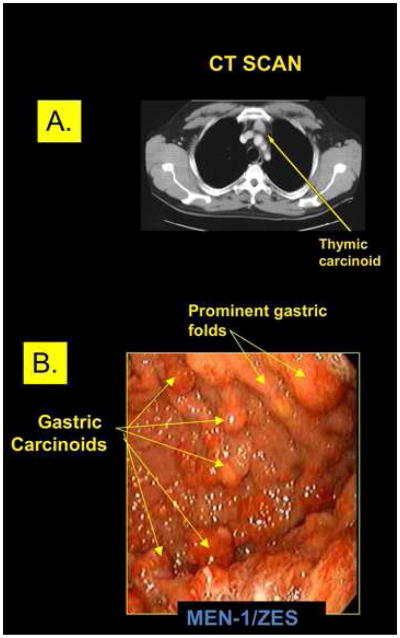
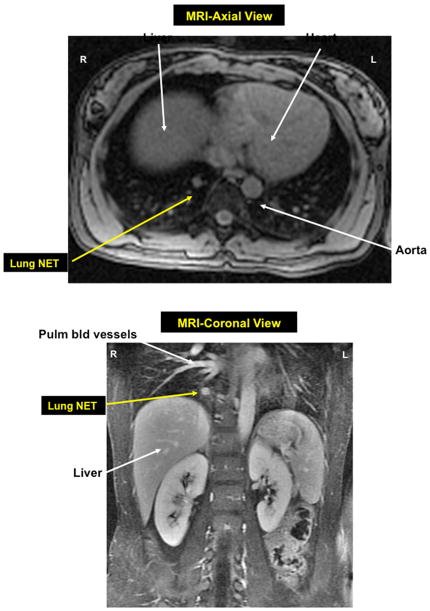
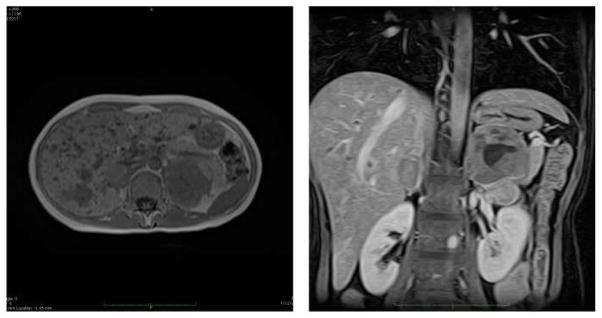
Early diagnosis of multiple endocrine neoplasia (MEN) syndromes is critical for optimal clinical outcomes; before the MEN syndromes can be diagnosed, they must be suspected. Genetic testing for germline alterations in both the MEN type 1 (MEN1) gene and RET proto-oncogene is crucial to identifying those at risk in affected kindreds and directing timely surveillance and surgical therapy to those at greatest risk of potentially life-threatening neoplasia. Pancreatic, thymic, and bronchial neuroendocrine tumors are the leading cause of death in patients with MEN1 and should be aggressively considered by at least biannual computed tomography imaging.
Keywords: Clinical management; Endocrine neoplasia; Genetics; Multiple endocrine neoplasia.
Copyright © 2015 Elsevier Inc. All rights reserved.
Figures

References
-
- Thakker RV, Newey PJ, Walls GV, Bilezikian J, Dralle H, Ebeling PR, Melmed S, Sakurai A, Tonelli F, Brandi ML. Clinical practice guidelines for multiple endocrine neoplasia type 1 (MEN1) J Clin Endocrinol Metab. 2012;97(9):2990–3011. - PubMed
-
- Giusti FCL, Cavalli T, Brandi ML. Hereditary hyperparathyroidism syndromes. J Clin Densitom. 2013;16(1):69–74. - PubMed
-
- Thakker RV. Multiple endocrine neoplasia type 1 (MEN1) Best Pract Res Clin Endocrinol Metab. 2010;24(3):355–370. - PubMed
-
- Brandi ML, Marx SJ, Aurbach GD, Fitzpatrick LA. Familial multiple endocrine neoplasia type I: a new look at pathophysiology. Endocr Rev. 1987;8(4):391–405. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
