

Regional Hospital Collaboration and Outcomes in Medicare Heart Failure Patients: See You in 7
- PMID: 26364256
- PMCID: PMC4701212
- DOI: 10.1016/j.jchf.2015.06.007
Regional Hospital Collaboration and Outcomes in Medicare Heart Failure Patients: See You in 7
Abstract
Objectives: The objective of this study was to evaluate an interhospital collaborative approach to improve 7-day post-discharge follow-up (7dFU) rates and reduce 30-day readmissions in heart failure (HF) patients.
Background: Early post-discharge follow-up after HF hospitalization is associated with lower 30-day readmission rates.
Methods: Observational analyses of Medicare HF patients discharged from 10 collaborating hospitals (CH) participating in the Southeast Michigan See You in 7 Collaborative were carried out. We compared pre-intervention (May 1, 2011 to April 30, 2012) and intervention (May 1, 2012 to April 30, 2013) 7dFU rates, unadjusted 30-day readmissions, risk-standardized 30-day readmissions (RSRR), and Medicare payments in CH and Michigan nonparticipating hospitals (NPH).
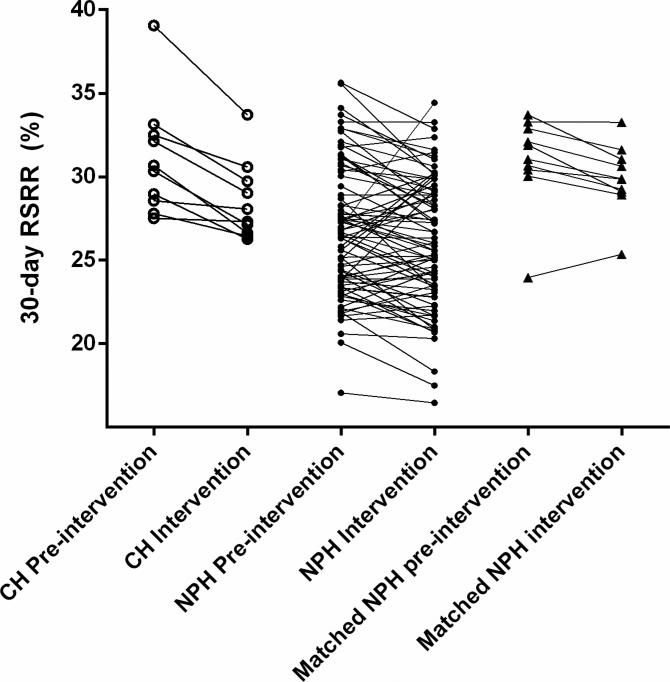
Results: 7dFU rates increased but remained low in both groups (CH: 31.1% to 34.4%; p < 0.001; NPH: 30.2% to 32.6%; p <0.001). During the intervention period, unadjusted readmissions decreased significantly in both groups (CH: 29.0% to 27.3%; p <0.001; NPH: 26.4% to 25.8%, p = 0.004); mean RSRR decreased more in CH than in NPH (CH: 31.1% to 28.5%; p < 0.001; NPH: 26.7% to 26.1%, p = 0.02; p = 0.015 for intergroup comparisons). Findings were similar when CH outcomes were matched 1:1 with similar NPH outcomes. Combined Medicare payments for inpatient and 30 days of post-discharge care decreased by $182 in CH and by $63 in NPH (per eligible HF discharge).
Conclusions: See You in 7 Collaborative participation was associated with significantly lower 30-day readmissions and Medicare payments in HF patients. Increases in 7dFU were modest, but associated processes aimed at this goal may have improved the transition from inpatient to outpatient care. Regional hospital collaboration to share best practices could potentially reduce HF readmissions and associated costs.
Keywords: care transitions; heart failure; outcomes; readmissions.
Copyright © 2015 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
What's Harder: Seeing a Doctor or Reducing Readmissions?JACC Heart Fail. 2015 Oct;3(10):774-6. doi: 10.1016/j.jchf.2015.07.004. Epub 2015 Sep 9. JACC Heart Fail. 2015. PMID: 26364258 No abstract available.
References
-
- Medicare Payment Advisory Commission . Report to the Congress: promoting greater efficiency in Medicare. MedPAC; Washington, DC: 2007. [October 2, 2013]. http://www.caretransitions.org/documents/MedPAC%20report.pdf.
-
- Henry J, Kaiser Family Foundation [September 15, 2014];The facts on Medicare spending and financing. 2014 Jul 28; http://kff.org/medicare/fact-sheet/medicare-spending-and-financing-fact-...
-
- Krumholz HM, Parent EM, Tu N, et al. Readmission after hospitalization for congestive heart failure among Medicare beneficiaries. Arch Intern Med. 1997;157:99–104. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
