

Two Cases of Pneumatoceles in Mechanically Ventilated Infants
- PMID: 26366266
- PMCID: PMC4561635
- DOI: 10.5001/omj.2015.59
Two Cases of Pneumatoceles in Mechanically Ventilated Infants
Abstract
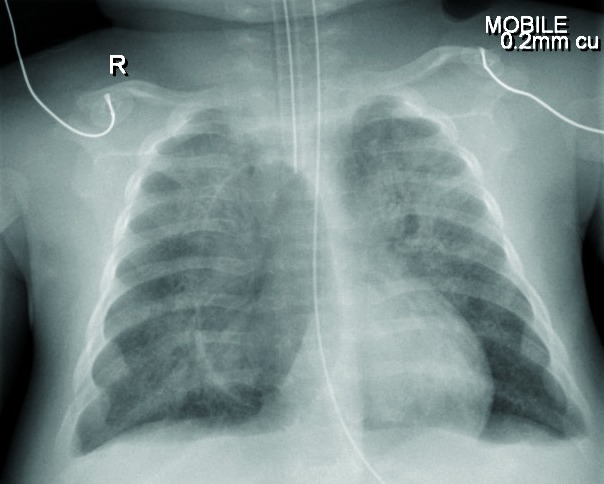
Pulmonary pneumatocele is a thin-walled, gas-filled space within the lung that usually occurs in association with bacterial pneumonia and is usually transient. The majority of pneumatoceles resolve spontaneously without active intervention, but in some cases they might lead to pneumothorax with subsequent hemodynamic instability. We report two cases presented to the pediatric intensive care unit at the Royal Hospital, Oman with pneumatoceles. The first was a 14-day-old baby who underwent surgical repair of total anomalous pulmonary venous connection (TAPVC) requiring extracorporeal membrane oxygenation (ECMO) support following surgery. He was initially on conventional mechanical ventilation. Seven days after the surgery, he started to develop bilateral pneumatoceles. The pneumatoceles were not regressing and they did not respond to three weeks of conservative management with high-frequency oscillation ventilation (HFOV). He failed four attempts of weaning from HFOV to conventional ventilation. Each time he was developing tachypnea and carbon dioxide retention. Percutaneous intercostal chest drain (ICD) insertion was needed to evacuate one large pneumatocele. Subsequently, he improved and we were able to wean and extubate him. The second case was a two-month-old male admitted with severe respiratory distress secondary to respiratory syncytial virus (RSV) pneumonitis. After intubation, he required a high conventional ventilation setting and within 24 hours he was on HFOV. Conservative management with HFOV was sufficient to treat the pneumatoceles and no further intervention was needed. Our cases demonstrate two different approaches in the management of pneumatoceles in mechanically ventilated children. Each approach was case dependent and could not be used interchangeably.
Keywords: Cardiopulmonary Bypass; Extracorporeal Membrane Oxygenation; High Frequency Oscillation Ventilation; Respiratory Syncytial Virus.
Figures


Similar articles
-
High frequency oscillation, extracorporeal membrane oxygenation and pumpless arteriovenous lung assist in the management of severe ARDS.Anestezjol Intens Ter. 2010 Oct-Dec;42(4):201-5. Anestezjol Intens Ter. 2010. PMID: 21252837
-
Effect of early intervention of high-frequency oscillatory ventilation on the outcome in pediatric acute respiratory distress syndrome.Bratisl Lek Listy. 2000;101(1):8-13. Bratisl Lek Listy. 2000. PMID: 10824405
-
Pneumatocele after lung transplantation.Gen Thorac Cardiovasc Surg Cases. 2023 Apr 11;2(1):10. doi: 10.1186/s44215-023-00030-9. Gen Thorac Cardiovasc Surg Cases. 2023. PMID: 39516888 Free PMC article.
-
Extra corporeal membrane oxygenation to facilitate lung protective ventilation and prevent ventilator-induced lung injury in severe Pneumocystis pneumonia with pneumomediastinum: a case report and short literature review.BMC Pulm Med. 2016 Apr 14;16(1):52. doi: 10.1186/s12890-016-0214-4. BMC Pulm Med. 2016. PMID: 27080997 Free PMC article. Review.
-
Elective high-frequency oscillatory ventilation versus conventional ventilation for acute pulmonary dysfunction in preterm infants.Neonatology. 2013;103(1):7-8; discussion 8-9. doi: 10.1159/000338553. Epub 2012 Aug 30. Neonatology. 2013. PMID: 23037971 Review.
Cited by
-
Post COVID-19 pneumo-hematocele: clinical presentation and treatment pathway.Gen Thorac Cardiovasc Surg. 2022 Jun;70(6):566-574. doi: 10.1007/s11748-022-01771-0. Epub 2022 Jan 18. Gen Thorac Cardiovasc Surg. 2022. PMID: 35041128 Free PMC article.
-
Pneumatocele formation following COVID-19 pneumonia. Is there a role for surgical intervention?Asian Cardiovasc Thorac Ann. 2021 Dec 7;30(4):2184923211059866. doi: 10.1177/02184923211059866. Online ahead of print. Asian Cardiovasc Thorac Ann. 2021. PMID: 34874785 Free PMC article.
References
-
- Nwokoro C, Issa M, Nastar A, Leigh M, Ross Russell R. Pneumatoceles following bronchiolitis in infancy: Worth a second look? ERS congress. September 20th, 2010.
-
- Plesca D, Hurduc V, Davitoiu A, Cavache A. Rare complication of acute bronchiolitis in infants: pneumatoceles. 15th ICID. Thailand; June 13-16, 2012.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical