

A unique biofilm in human deep mycoses: fungal amyloid is bound by host serum amyloid P component
- PMID: 26366292
- PMCID: PMC4563996
- DOI: 10.1038/npjbiofilms.2015.9
A unique biofilm in human deep mycoses: fungal amyloid is bound by host serum amyloid P component
Abstract
Background/objectives: We have demonstrated the presence of Candida cell surface amyloids that are important in aggregation of fungi and adherence to tissue. Fungal amyloid was present in invasive human candidal infections and host serum amyloid P component (SAP) bound to the fungal amyloid. SAP is a protease-resistant glycoprotein that binds avidly to amyloid and interferes with host defence, especially against bacterial pathogens for which neutrophils are important. In this study, we investigated whether biofilm of fungal amyloid and SAP was a feature of other disseminated fungal infections.
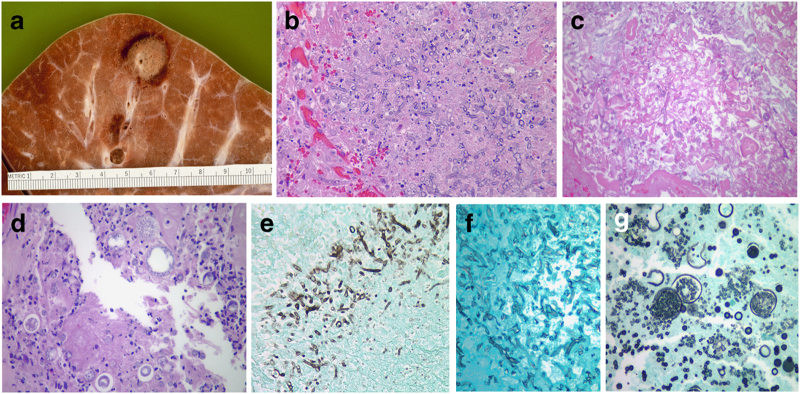
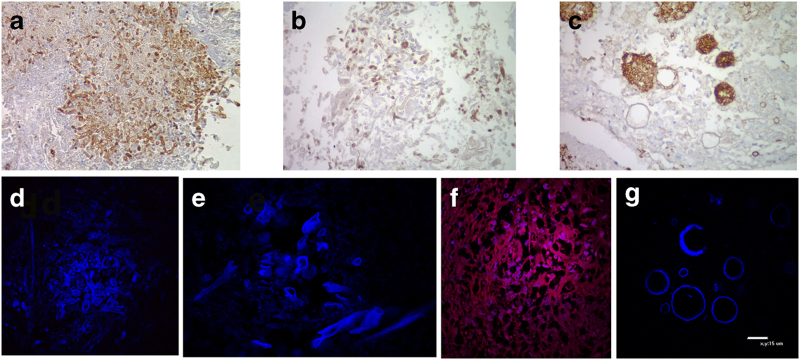
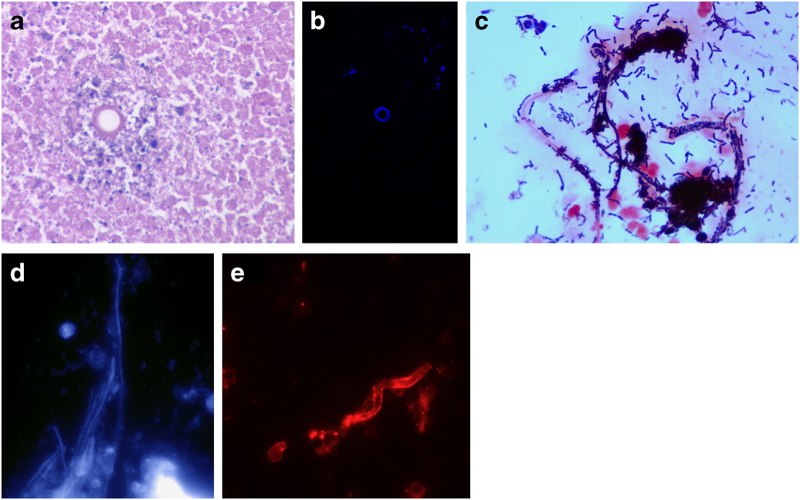
Methods: Tissue specimens from 15 autopsies were systematically evaluated with multiple histochemical stains including thioflavin T and Congo red (dyes that stain amyloid), as well as antibody to SAP. We studied specimens with disseminated aspergillosis, mucormycosis and coccidioidomycosis. The structure of the lesions, host inflammatory cells and the presence of fungal amyloid and SAP were determined.
Results: The structure of the lesions was characteristic in aspergillosis ('starburst') and mucormycosis (closely apposed bundles of hyphae). Host inflammatory cells were absent or few in number within these lesions. In Coccidioides lesions, host inflammation was sparse as well. Fungal amyloid was a prominent feature of all lesions along with abundant SAP bound to hyphae and spherules. Fungal amyloid and SAP perhaps contributed to persistence in caseous necrosis lesions. SAP also bound to Aspergillus and Mucorales amyloid in vitro.
Conclusions: A biofilm including amyloid and SAP is present in invasive fungal infections. This biofilm may dampen host defence leading to the characteristic sparse inflammatory reaction found in these infections.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Berenguer J , Allende MC , Lee JW , Garrett K , Lyman C , Ali NM et al. Pathogenesis of pulmonary aspergillus. Granulocytopenia versus cyclosporine and methylprednisolone-induced immunosuppression. Am J Resp Crit Care Med 1995; 152: 1079–1086. - PubMed
-
- Stergiopoulou T , Meletiadis J , Rollides E , Kleiner DE , Schaufele R , Roden M et al. Host-dependent patterns of tissue injury in invasive pulmonary aspergillosis. Am J Clin Pathol 2007; 127: 349–355. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
