

Relationship Between Margin Width and Recurrence of Ductal Carcinoma In Situ: Analysis of 2996 Women Treated With Breast-conserving Surgery for 30 Years
- PMID: 26366541
- PMCID: PMC4739638
- DOI: 10.1097/SLA.0000000000001454
Relationship Between Margin Width and Recurrence of Ductal Carcinoma In Situ: Analysis of 2996 Women Treated With Breast-conserving Surgery for 30 Years
Abstract
Objective: Our goal was to investigate, in a large population of women with ductal carcinoma in situ (DCIS) and long follow-up, the relationship between margin width and recurrence, controlling for other characteristics.
Background: Although DCIS has minimal mortality, recurrence rates after breast-conserving surgery are significant, and half are invasive. Positive margins are associated with increased risk of local recurrence, but there is no consensus regarding optimal negative margin width.
Methods: We retrospectively reviewed a prospective database of DCIS patients undergoing breast-conserving surgery from 1978 to 2010. Univariate and Cox proportional hazard models were used to investigate the association between margin width and recurrence.
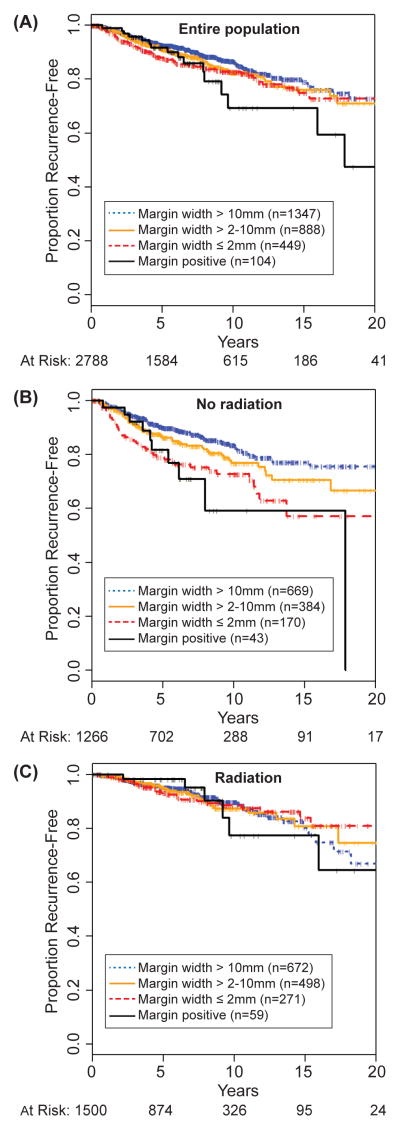
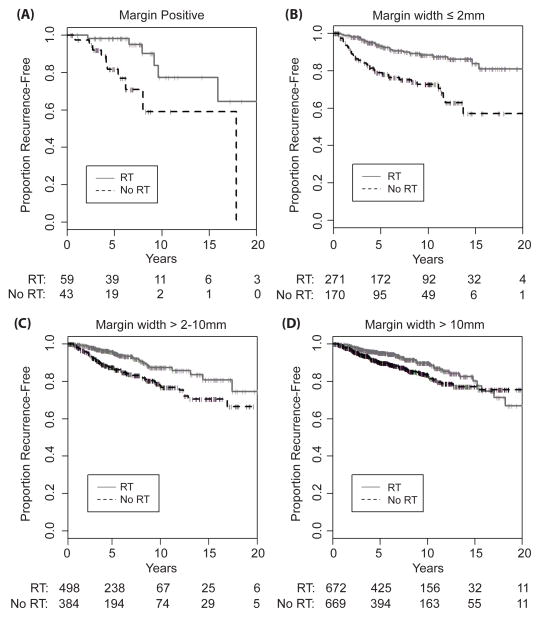
Results: In this review, 2996 cases were identified, of which 363 recurred. Median follow-up for women without recurrence was 75 months (range 0-30 years); 732 were studied for ≥10 years. Controlling for age, family history, presentation, nuclear grade, number of excisions, radiotherapy (RT), endocrine therapy, and year of surgery, margin width was significantly associated with recurrence in the entire population. Larger negative margins were associated with a lower hazard ratio compared with positive margins. An interaction between RT and margin width was significant (P < 0.03); the association of recurrence with margin width was significant in those without RT (P < 0.0001), but not in those with RT (P = 0.95).
Conclusions: In women not receiving RT, wider margins are significantly associated with a lower rate of recurrence. Obtaining wider negative margins may be important in reducing the risk of recurrence in women who choose not to undergo RT and may not be necessary in those who receive RT.
Figures
Comment in
-
ASO Author Reflections: Does Genomic Testing of DCIS Provide Added Value? And Is It Worth the Cost?Ann Surg Oncol. 2019 Dec;26(Suppl 3):702-703. doi: 10.1245/s10434-019-07745-6. Epub 2019 Aug 23. Ann Surg Oncol. 2019. PMID: 31444602 Free PMC article. No abstract available.
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA: A Cancer Journal for Clinicians. 2015;65:5–29. - PubMed
-
- Donker M, Litiere S, Werutsky G, et al. Breast-conserving treatment with or without radiotherapy in ductal carcinoma In Situ: 15-year recurrence rates and outcome after a recurrence, from the EORTC 10853 randomized phase III trial. J Clin Oncol. 2013;31:4054–4059. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
