

Effect of Antiretroviral Therapy on HIV-mediated Impairment of the Neutrophil Antimycobacterial Response
- PMID: 26368270
- PMCID: PMC4724897
- DOI: 10.1513/AnnalsATS.201507-463OC
Effect of Antiretroviral Therapy on HIV-mediated Impairment of the Neutrophil Antimycobacterial Response
Abstract
Rationale: Experimental and epidemiological evidence suggests that neutrophils are important in the host response to tuberculosis. HIV infection, which increases the risk of tuberculosis, adversely affects neutrophil function.
Objectives: To determine the impact of HIV and antiretroviral therapy on neutrophil antimycobacterial activity.
Methods: We performed a cross-sectional comparison of neutrophil functions in 20 antiretroviral-naive HIV-infected and 20 HIV-uninfected individuals using luminescence-, flow cytometry-, and ELISA-based assays. We then conducted a prospective study in the HIV-infected individuals investigating these parameters during the first 6 months of antiretroviral therapy. Surface markers of neutrophil activation were investigated in a separate cohort using flow cytometry.
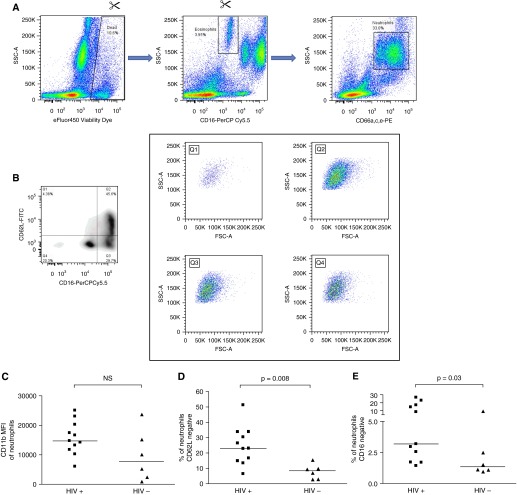
Measurements and main results: HIV infection impaired control of Mycobacterium tuberculosis by neutrophils (mean ratio of mycobacterial luminescence in neutrophil samples vs. serum controls at 1 hour in HIV-infected participants, 0.88 ± 0.13 vs. HIV-uninfected participants, 0.76 ± 0.14; P = 0.01; at 24 hours, 0.82 ± 0.13 vs. 0.71 ± 0.13; P = 0.01). The extent of impairment correlated with log[HIV viral load]. Neutrophil cell death after 24 hours' incubation with M. tuberculosis was higher in the HIV-infected cohort (85.3 ± 11.8% vs. 57.9 ± 22.4% necrotic cells; P < 0.0001). Neutrophils from HIV-infected participants demonstrated significantly more CD62L-negative cells (median, 23.0 vs. 8.5%; P = 0.008) and CD16-negative cells (3.2 vs. 1.3%, P = 0.03). Antiretroviral therapy restored mycobacterial restriction and pattern of neutrophil death toward levels seen in HIV-uninfected persons.
Conclusions: Neutrophils in antiretroviral-naive HIV-infected persons are hyperactivated, eliminate M. tuberculosis less effectively than in HIV-uninfected individuals, and progress rapidly to necrotic cell death. These factors are ameliorated by antiretroviral therapy.
Keywords: granulocyte; necrosis; tuberculosis.
Figures



References
-
- World Health Organization. Global Health Observatory (GHO) data. How many TB cases and deaths are there? [accessed 2015 Jan]. Available from: www.who.int/gho/tb/epidemic/cases_deaths/en/
-
- World Health Organization. Global Health Observatory (GHO) Data. Number of deaths due to HIV/AIDS [accessed 2015 Jan] Available from: http://www.who.int/gho/hiv/epidemic_status/deaths/en/
-
- Lawn SD. AIDS in Africa: the impact of coinfections on the pathogenesis of HIV-1 infection. J Infect. 2004;48:1–12. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
