

Non-invasive screening of diabetics in primary care for NAFLD and advanced fibrosis by MRI and MRE
- PMID: 26369383
- PMCID: PMC4673036
- DOI: 10.1111/apt.13405
Non-invasive screening of diabetics in primary care for NAFLD and advanced fibrosis by MRI and MRE
Abstract
Background: Current guidelines do not recommend screening for non-alcoholic fatty liver disease (NAFLD) or advanced fibrosis. Patients with type 2 diabetes mellitus (T2DM) are known to be at increased risk for NAFLD and advanced fibrosis.
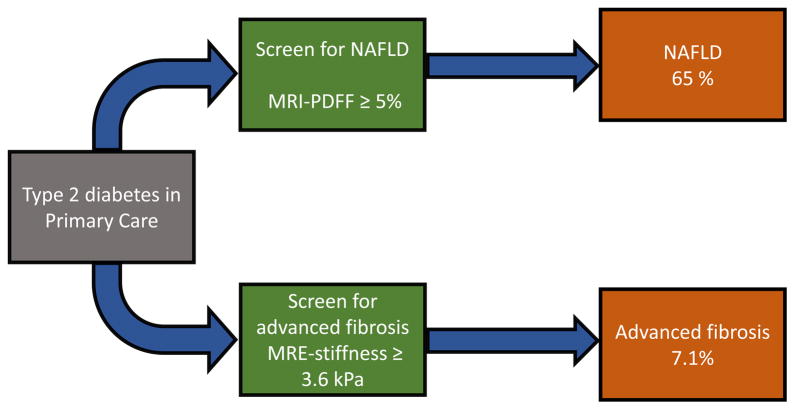
Aim: To assess the feasibility in diabetics in a primary care setting of screening for NAFLD and advanced fibrosis, by using non-invasive magnetic resonance imaging (MRI) to estimate the hepatic proton density fat fraction (MRI-PDFF) and magnetic resonance elastography (MRE) to estimate hepatic stiffness.
Methods: We performed a cross-sectional analysis of a prospective study that included 100 (53% men) consecutively enrolled diabetics who did not have any other aetiology of liver disease. All patients underwent a standardised research visit, laboratory tests, MRI-PDFF, and MRE.
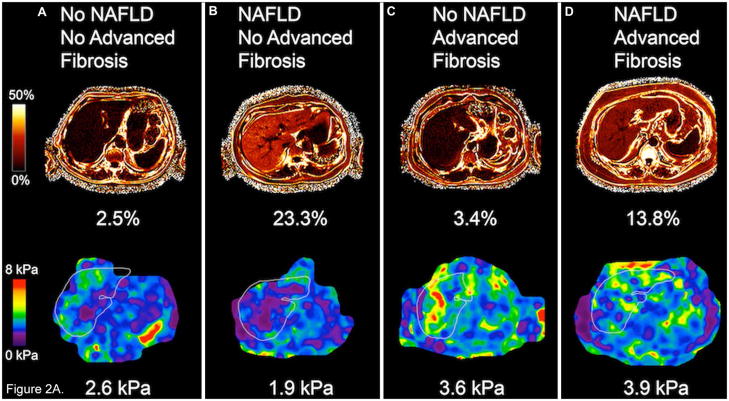
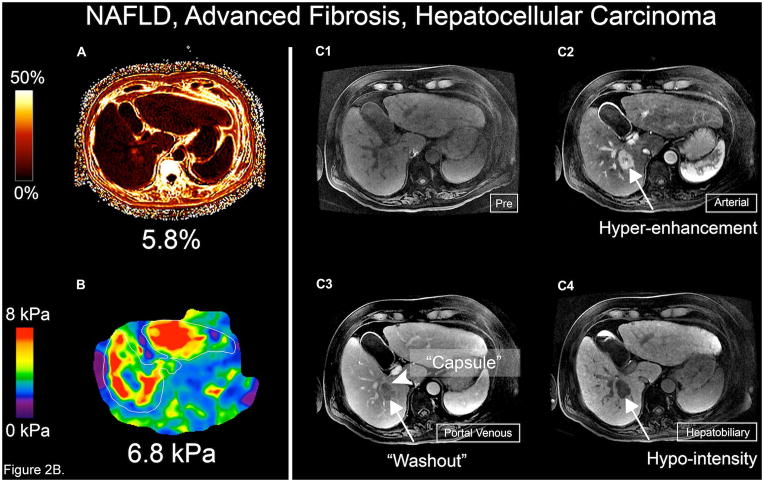
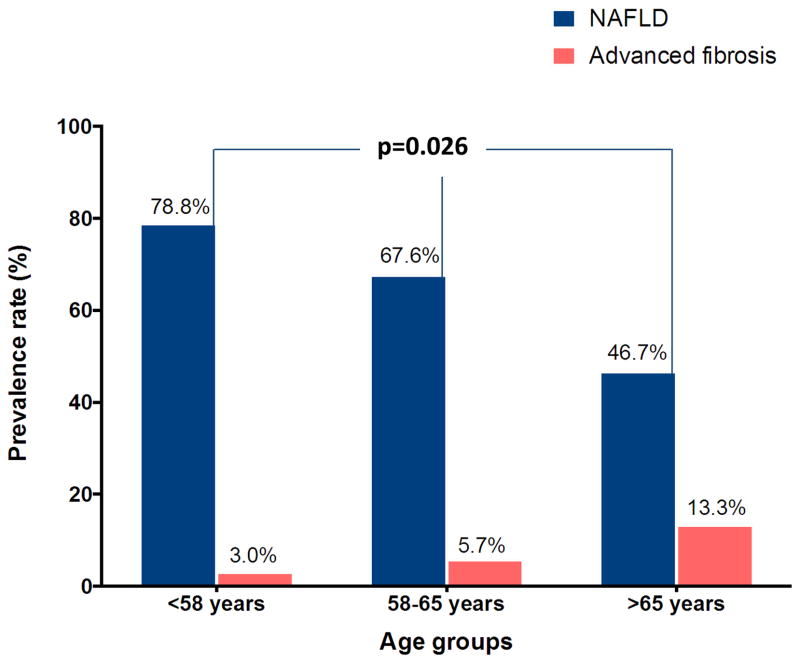
Results: Mean (±s.d.) age and body mass index (BMI) was 59.7 (±11.2) years and 30.8 (±6.5) kg/m(2) , respectively. The prevalence of NAFLD (defined as MRI-PDFF ≥5%) and advanced fibrosis (defined as MRE ≥3.6 kPa) was 65% and 7.1%, respectively. One patient with advanced fibrosis had definite hepatocellular carcinoma. When compared to those without NAFLD, patients with NAFLD were younger (P = 0.028) and had higher mean BMI (P = 0.0008), waist circumference (P < 0.0001) and prevalence of metabolic syndrome (84.6% vs. 40.0%, P < 0.0001). Only 26% of those with NAFLD had elevated alanine aminotransferase.
Conclusions: This proof-of-concept study demonstrates that T2DM has significant rates of both NAFLD and advanced fibrosis. Concomitant screening for NAFLD and advanced fibrosis by using MRI-proton density fat fraction and magnetic resonance elastography in T2DM is feasible and may be considered after validation in a larger cohort.
© 2015 John Wiley & Sons Ltd.
Conflict of interest statement
All authors report no conflicts of interest.
Figures
Comment in
-
Editorial: screening for NAFLD - a promising strategy to mitigate future burden of liver disease.Aliment Pharmacol Ther. 2016 Jan;43(1):163. doi: 10.1111/apt.13421. Aliment Pharmacol Ther. 2016. PMID: 26638929 No abstract available.
References
-
- Williams CD, Stengel J, Asike MI, et al. Prevalence of nonalcoholic fatty liver disease and nonalcoholic steatohepatitis among a largely middle-aged population utilizing ultrasound and liver biopsy: a prospective study. Gastroenterology. 2011;140:124–31. - PubMed
-
- Cusi K. Role of insulin resistance and lipotoxicity in non-alcoholic steatohepatitis. Clin Liver Dis. 2009;13:545–63. - PubMed
-
- Targher G, Bertolini L, Padovani R, et al. Prevalence of nonalcoholic fatty liver disease and its association with cardiovascular disease among type 2 diabetic patients. Diabetes Care. 2007;30:1212–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical