

Colistin Population Pharmacokinetics after Application of a Loading Dose of 9 MU Colistin Methanesulfonate in Critically Ill Patients
- PMID: 26369974
- PMCID: PMC4649253
- DOI: 10.1128/AAC.00554-15
Colistin Population Pharmacokinetics after Application of a Loading Dose of 9 MU Colistin Methanesulfonate in Critically Ill Patients
Abstract
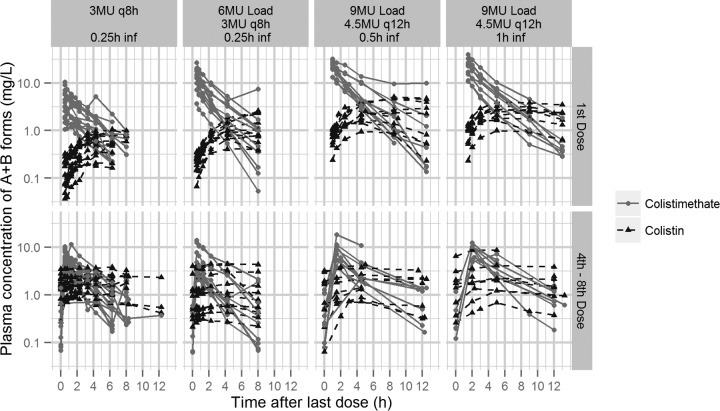
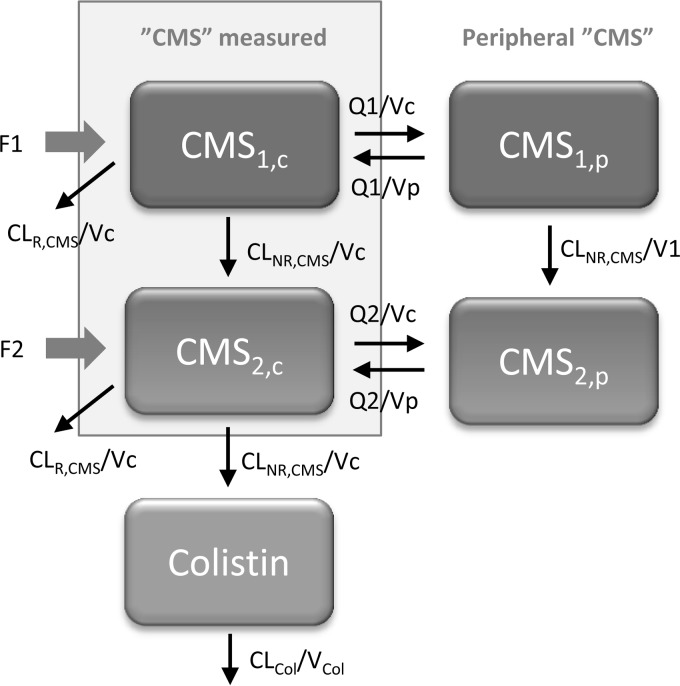
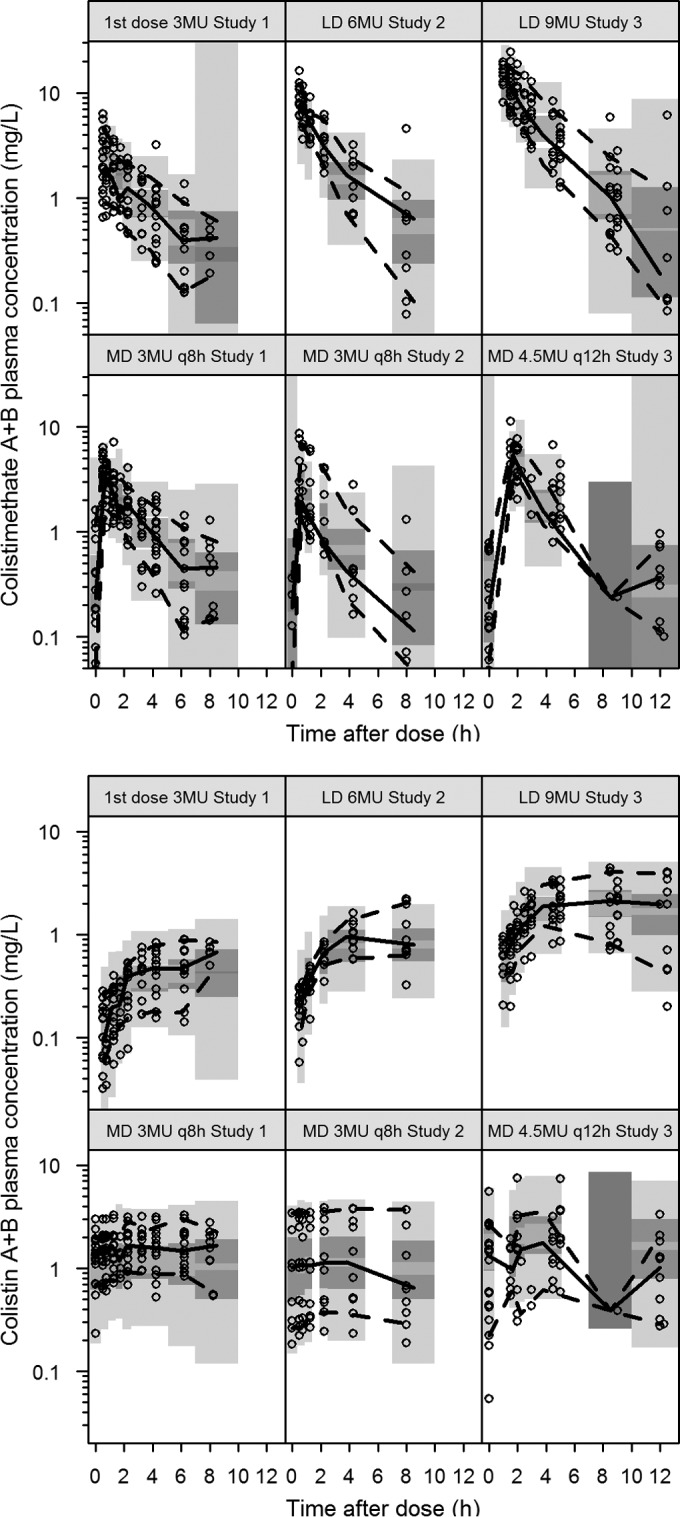
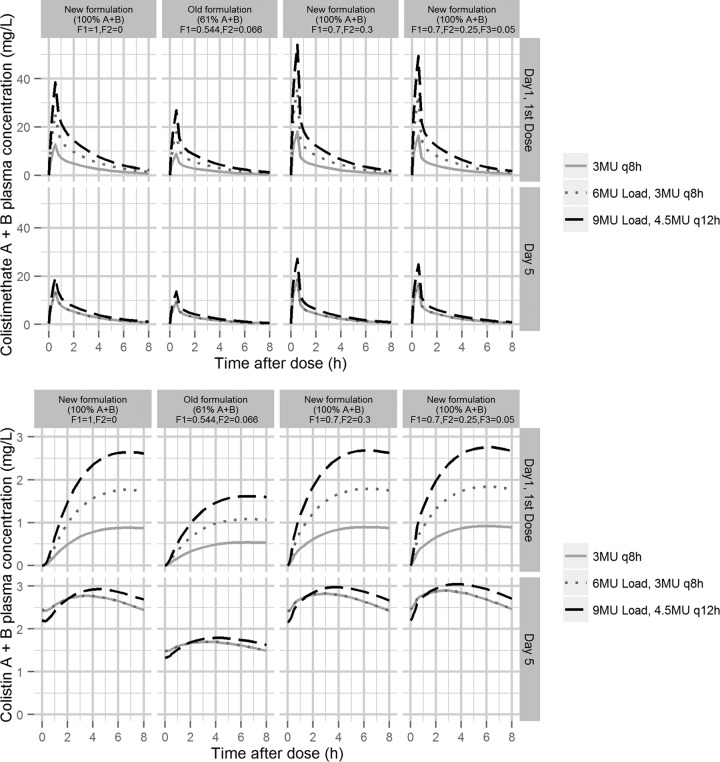
Colistin has been revived, in the era of extensively drug-resistant (XDR) Gram-negative infections, as the last-resort treatment in critically ill patients. Recent studies focusing on the optimal dosing strategy of colistin have demonstrated the necessity of a loading dose at treatment initiation (D. Plachouras, M. Karvanen, L. E. Friberg, E. Papadomichelakis, A. Antoniadou, I. Tsangaris, I. Karaiskos, G. Poulakou, F. Kontopidou, A. Armaganidis, O. Cars, and H. Giamarellou, Antimicrob Agents Chemother 53:3430-3436, 2009, http://dx.doi.org/10.1128/AAC.01361-08; A. F. Mohamed, I. Karaiskos, D. Plachouras, M. Karvanen, K. Pontikis, B. Jansson, E. Papadomichelakis, A. Antoniadou, H. Giamarellou, A. Armaganidis, O. Cars, and L. E. Friberg, Antimicrob Agents Chemother 56:4241- 4249, 2012, http://dx.doi.org/10.1128/AAC.06426-11; S. M. Garonzik, J. Li, V. Thamlikitkul, D. L. Paterson, S. Shoham, J. Jacob, F. P. Silveira, A. Forrest, and R. L. Nation, Antimicrob Agents Chemother 55:3284-3294, 2011, http://dx.doi.org/10.1128/AAC.01733-10). In 19 critically ill patients with suspected or microbiologically documented infections caused by XDR Gram-negative strains, a loading dose of 9 MU colistin methanesulfonate (CMS) (∼ 270 mg colistin base activity) was administered with a maintenance dose of 4.5 MU every 12 h, commenced after 24 h. Patients on renal replacement were excluded. CMS infusion was given over 30 min or 1 h. Repeated blood sampling was performed after the loading dose and after the 5th or 6th dose. Colistin concentrations and measured CMS, determined after hydrolization to colistin and including the partially sulfomethylated derivatives, were determined with a liquid chromatography-tandem mass spectrometry assay. Population pharmacokinetic analysis was conducted in NONMEM with the new data combined with data from previous studies. Measured colistimethate concentrations were described by 4 compartments for distribution and removal of sulfomethyl groups, while colistin disposition followed a 1-compartment model. The average observed maximum colistin A plus B concentration was 2.65 mg/liter after the loading dose (maximum time was 8 h). A significantly higher availability of the measured A and B forms of colistimethate and colistin explained the higher-than-expected concentrations in the present study compared to those in previous studies. Creatinine clearance was a time-varying covariate of colistimethate clearance. The incidence of acute renal injury was 20%.
Copyright © 2015, American Society for Microbiology. All Rights Reserved.
Figures
References
-
- World Health Organization (WHO). 2011. Antimicrobial resistance: no action today, no cure tomorrow. WHO Press, Geneva, Switzerland: http://www.who.int/world-health-day/2011/en/index.html.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
