

Persistently Altered Brain Mitochondrial Bioenergetics After Apparently Successful Resuscitation From Cardiac Arrest
- PMID: 26370446
- PMCID: PMC4599507
- DOI: 10.1161/JAHA.115.002232
Persistently Altered Brain Mitochondrial Bioenergetics After Apparently Successful Resuscitation From Cardiac Arrest
Abstract
Background: Although advances in cardiopulmonary resuscitation have improved survival from cardiac arrest (CA), neurologic injury persists and impaired mitochondrial bioenergetics may be critical for targeted neuroresuscitation. The authors sought to determine if excellent cardiopulmonary resuscitation and postresuscitation care and good traditional survival rates result in persistently disordered cerebral mitochondrial bioenergetics in a porcine pediatric model of asphyxia-associated ventricular fibrillation CA.
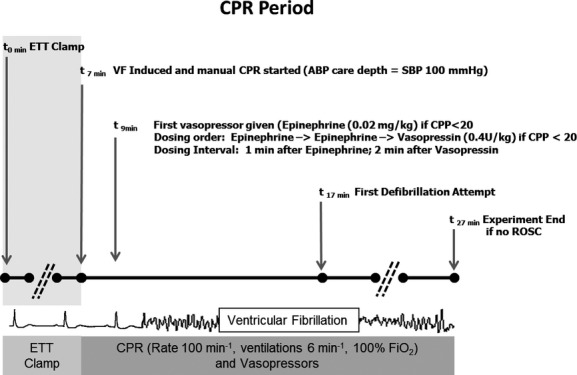
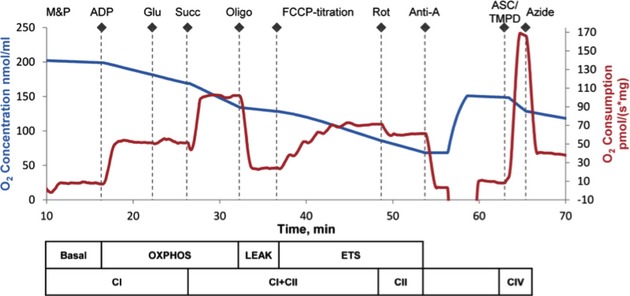
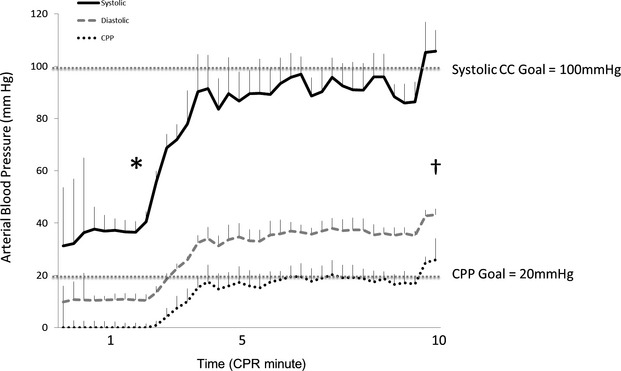
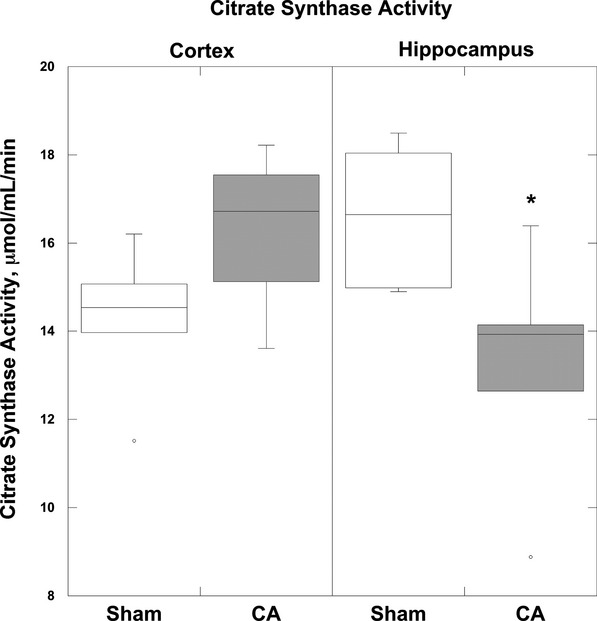
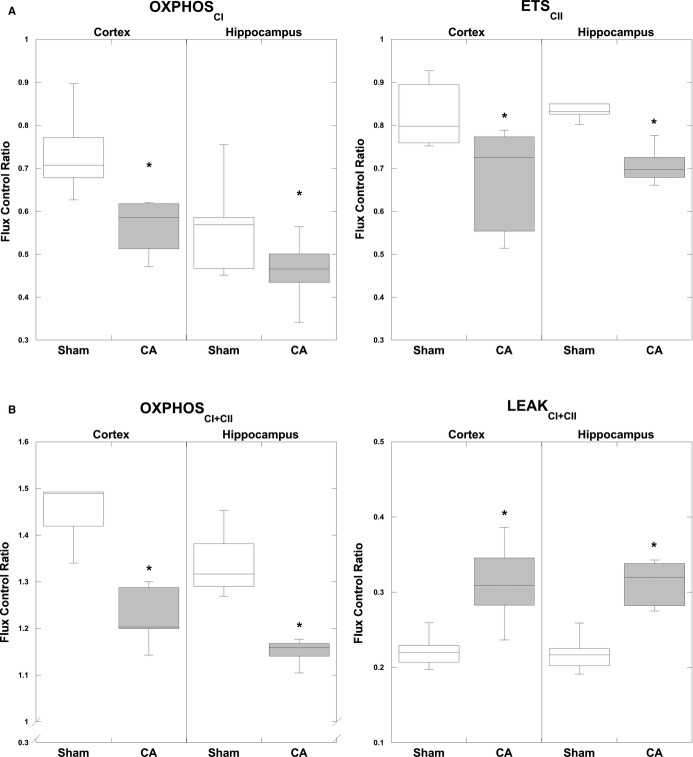
Methods and results: After 7 minutes of asphyxia, followed by ventricular fibrillation, 5 female 1-month-old swine (4 sham) received blood pressure-targeted care: titration of compression depth to systolic blood pressure of 90 mm Hg and vasopressor administration to a coronary perfusion pressure >20 mm Hg. All animals received protocol-based vasopressor support after return of spontaneous circulation for 4 hours before they were killed. The primary outcome was integrated mitochondrial electron transport system (ETS) function. CA animals displayed significantly decreased maximal, coupled oxidative phosphorylating respiration (OXPHOSCI + CII) in cortex (P<0.02) and hippocampus (P<0.02), as well as decreased phosphorylation and coupling efficiency (cortex, P<0.05; hippocampus, P<0.05). Complex I- and complex II-driven respiration were both significantly decreased after CA (cortex: OXPHOSCI P<0.01, ETSCII P<0.05; hippocampus: OXPHOSCI P<0.03, ETSCII P<0.01). In the hippocampus, there was a significant decrease in maximal uncoupled, nonphosphorylating respiration (ETSCI + CII), as well as a 30% reduction in citrate synthase activity (P<0.04).
Conclusions: Mitochondria in both the cortex and hippocampus displayed significant alterations in respiratory function after CA despite excellent cardiopulmonary resuscitation and postresuscitation care in asphyxia-associated ventricular fibrillation CA. Analysis of integrated ETS function identifies mitochondrial bioenergetic failure as a target for goal-directed neuroresuscitation after CA. IACUC Protocol: IAC 13-001023.
Keywords: acute brain injury; brain; cardiac arrest; electron transport system; mitochondria; neuroprotection.
© 2015 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Merchant RM, Yang L, Becker LB, Berg RA, Nadkarni V, Nichol G, Carr BG, Mitra N, Bradley SM, Abella BS, Groeneveld PW American Heart Association Get With The Guidelines-Resuscitation Investigators. Incidence of treated cardiac arrest in hospitalized patients in the United States. Crit Care Med. 2011;39:2401–2406. - PMC - PubMed
-
- Girotra S, Chan PS. Trends in survival after in-hospital cardiac arrest. N Engl J Med. 2013;368:680–681. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
