

Comparison of mandibular cortical thickness and QCT-derived bone mineral density (BMD) in survivors of childhood acute lymphoblastic leukemia: a retrospective study
- PMID: 26370921
- PMCID: PMC4792795
- DOI: 10.1111/ipd.12203
Comparison of mandibular cortical thickness and QCT-derived bone mineral density (BMD) in survivors of childhood acute lymphoblastic leukemia: a retrospective study
Abstract
Objective: To examine whether panoramic radiograph-determined mandibular cortical thickness correlated with quantitative computed tomography-derived bone mineral density (BMD) in survivors of childhood acute lymphoblastic leukemia (ALL).
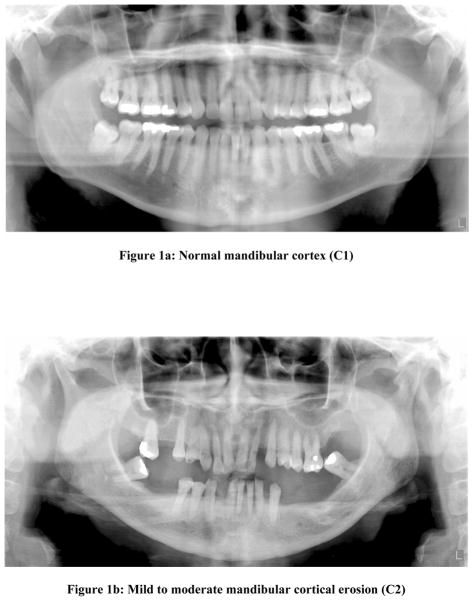
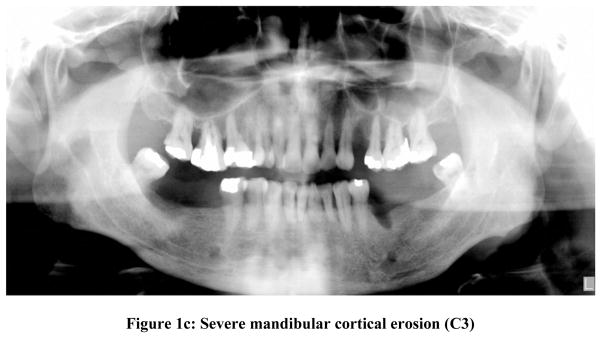
Methods: We identified patients treated for ALL at St. Jude Children's Research Hospital, seen in the After Completion of Therapy (ACT) Clinic between January of 2006 and January of 2014 who had QCT-derived BMD and panoramic radiographs obtained within 1 month of each other. Panoramic radiographs were independently scored by a pediatric radiologist, two pediatric dentists, and a general dentist using the Klemetti technique. We used the Spearman's rank correlation test and the multivariate regression model to investigate the effect of evaluator experience on results.
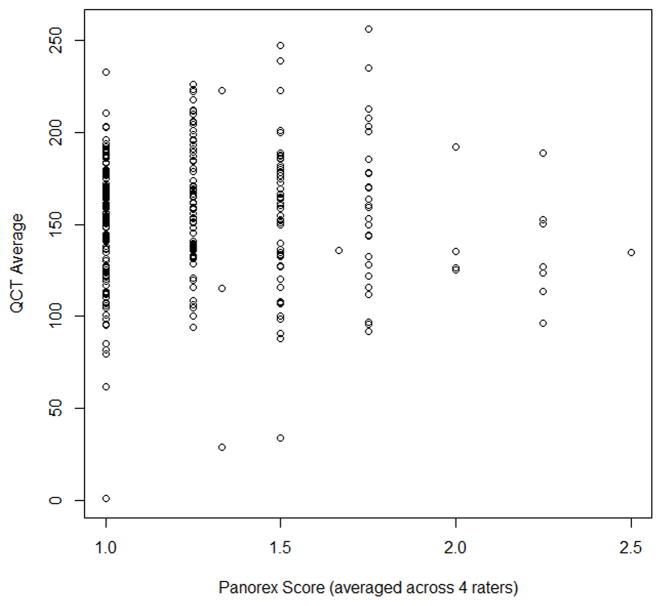
Results: The study cohort comprised 181 patients with 320 paired studies: 112 (62%) male, 112 (71%) were white. Median age at ALL diagnosis was 6.4 (range, 0-18.8) years. Median age at study was 11.9 (range, 3.3 to 29.4) years. The median average BMD was 154.6 (range, 0.73-256) mg/cc; median QCT Z-score (age and gender adjusted) was -0.875 (range, -5.04 to 3.2). We found very weak association between panoramic radiograph score and both QCT-BMD average (P = 0.53) and QCT Z-score (P = 0.39). Results were not influenced by level of reader experience.
Conclusions: The Klemetti technique of estimating BMD does not predict BMD deficits in children and young adult survivors of ALL, regardless of reviewer expertise. Alternative methods are needed whereby dental healthcare providers can identify and refer patients at risk for BMD deficits for detailed assessment and intervention.
© 2015 BSPD, IAPD and John Wiley & Sons A/S. Published by John Wiley & Sons Ltd.
Figures
References
-
- Kaste SC, Jones-Wallace D, Rose SR, et al. Bone mineral decrements in survivors of childhood acute lymphoblastic leukemia: frequency of occurrence and risk factors for their development. Leukemia. 2001;15(5):728–34. - PubMed
-
- Kaste SC, Rai SN, Fleming K, et al. Changes in bone mineral density in survivors of childhood acute lymphoblastic leukemia. Pediatr Blood Cancer. 2006;46(1):77–87. - PubMed
-
- Atkinson SA, Halton JM, Bradley C, Wu B, Barr RD. Bone and mineral abnormalities in childhood acute lymphoblastic leukemia: influence of disease, drugs and nutrition. Int J Cancer Suppl. 1998;11:35–9. - PubMed
-
- Boot AM, van den Heuvel-Eibrink MM, Hahlen K, Krenning EP, de Muinck Keizer-Schrama SM. Bone mineral density in children with acute lymphoblastic leukaemia. Eur J Cancer. 1999;35(12):1693–7. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
