

Alopecia areata: Part 1: pathogenesis, diagnosis, and prognosis
- PMID: 26371097
- PMCID: PMC4569104
Alopecia areata: Part 1: pathogenesis, diagnosis, and prognosis
Abstract
Objective: To provide family physicians with a background understanding of the epidemiology, pathogenesis, histology, and clinical approach to the diagnosis of alopecia areata (AA).
Sources of information: PubMed was searched for relevant articles regarding the pathogenesis, diagnosis, and prognosis of AA.
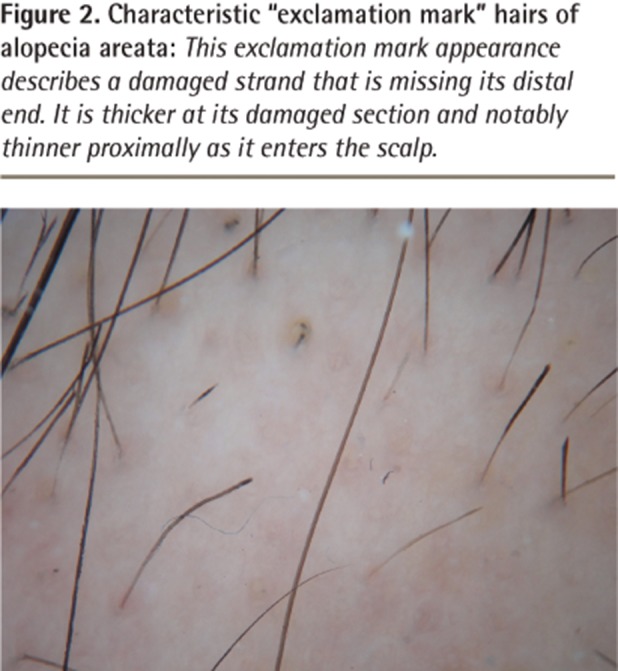
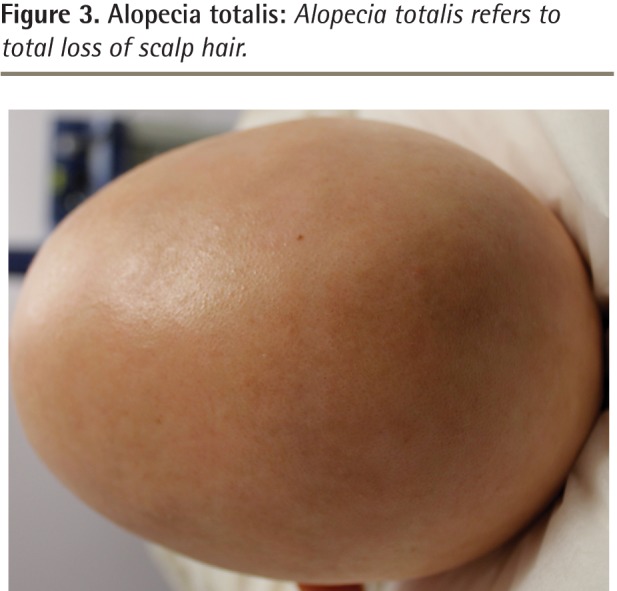
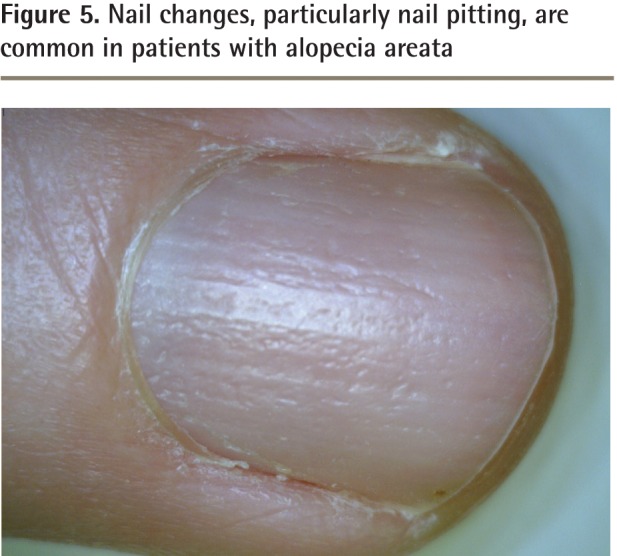
Main message: Alopecia areata is a form of autoimmune hair loss with a lifetime prevalence of approximately 2%. A personal or family history of concomitant autoimmune disorders, such as vitiligo or thyroid disease, might be noted in a small subset of patients. Diagnosis can often be made clinically, based on the characteristic nonscarring, circular areas of hair loss, with small "exclamation mark" hairs at the periphery in those with early stages of the condition. The diagnosis of more complex cases or unusual presentations can be facilitated by biopsy and histologic examination. The prognosis varies widely, and poor outcomes are associated with an early age of onset, extensive loss, the ophiasis variant, nail changes, a family history, or comorbid autoimmune disorders.
Conclusion: Alopecia areata is an autoimmune form of hair loss seen regularly in primary care. Family physicians are well placed to identify AA, characterize the severity of disease, and form an appropriate differential diagnosis. Further, they are able educate their patients about the clinical course of AA, as well as the overall prognosis, depending on the patient subtype.
Copyright© the College of Family Physicians of Canada.
Figures


References
-
- Safavi K. Prevalence of alopecia areata in the First National Health and Nutrition Examination Survey. Arch Dermatol. 1992;128(5):702. - PubMed
-
- Safavi KH, Muller SA, Suman VJ, Moshell AN, Melton LJ., 3rd Incidence of alopecia areata in Olmsted County, Minnesota, 1975 through 1989. Mayo Clin Proc. 1995;70(7):628–33. - PubMed
-
- Shellow WV, Edwards JE, Koo JY. Profile of alopecia areata: a questionnaire analysis of patient and family. Int J Dermatol. 1992;31(3):186–9. - PubMed
-
- Kyriakis KP, Paltatzidou K, Kosma E, Sofouri E, Tadros A, Rachioti E. Alopecia areata prevalence by gender and age. J Eur Acad Dermatol Venereol. 2009;23(5):572–3. Epub 2008 Sep 8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources