

Neither classical nor alternative macrophage activation is required for Pneumocystis clearance during immune reconstitution inflammatory syndrome
- PMID: 26371121
- PMCID: PMC4645389
- DOI: 10.1128/IAI.00763-15
Neither classical nor alternative macrophage activation is required for Pneumocystis clearance during immune reconstitution inflammatory syndrome
Abstract
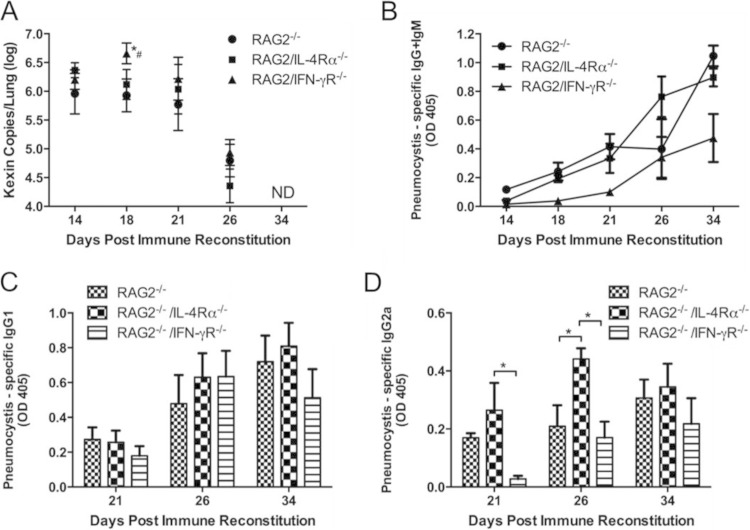
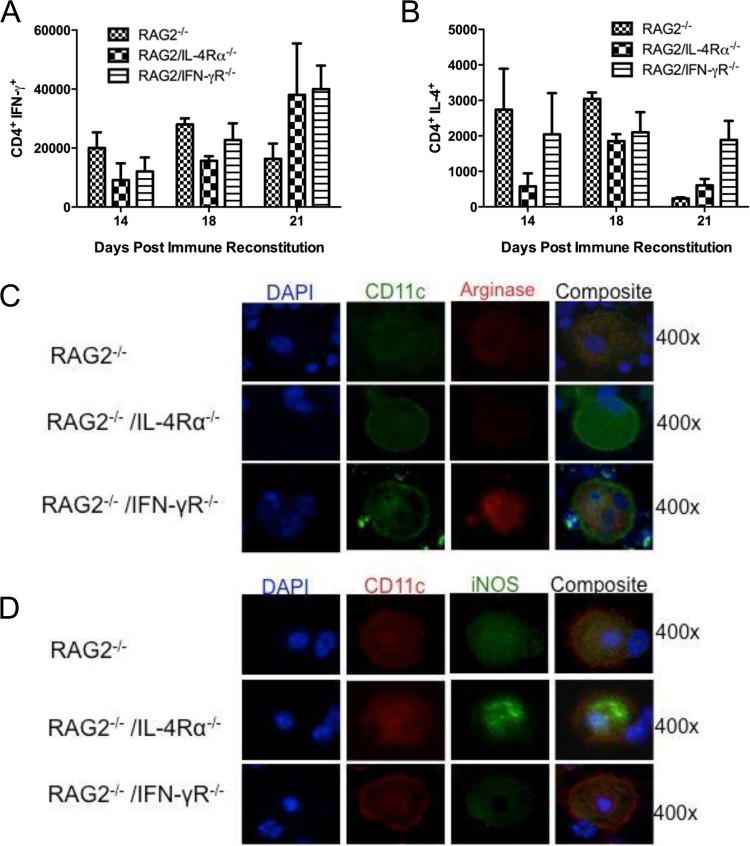
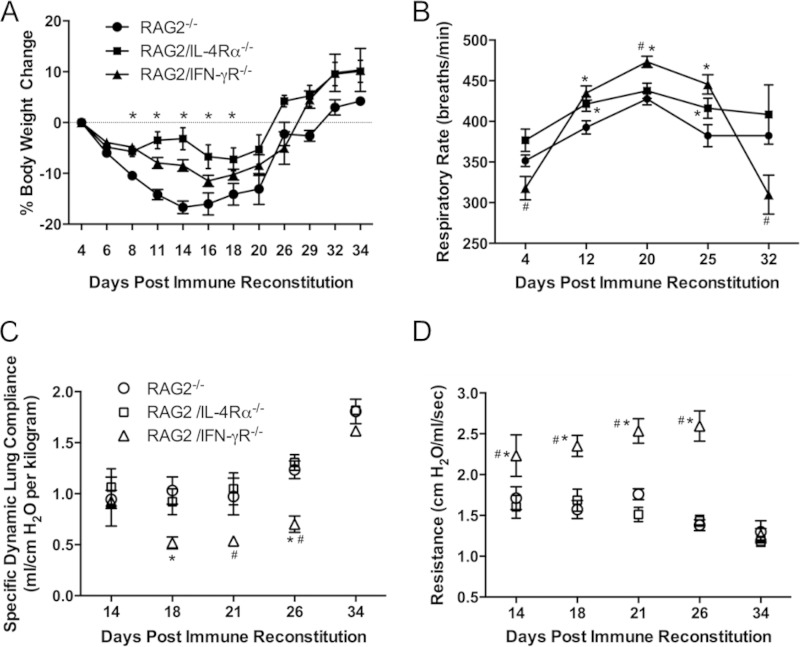
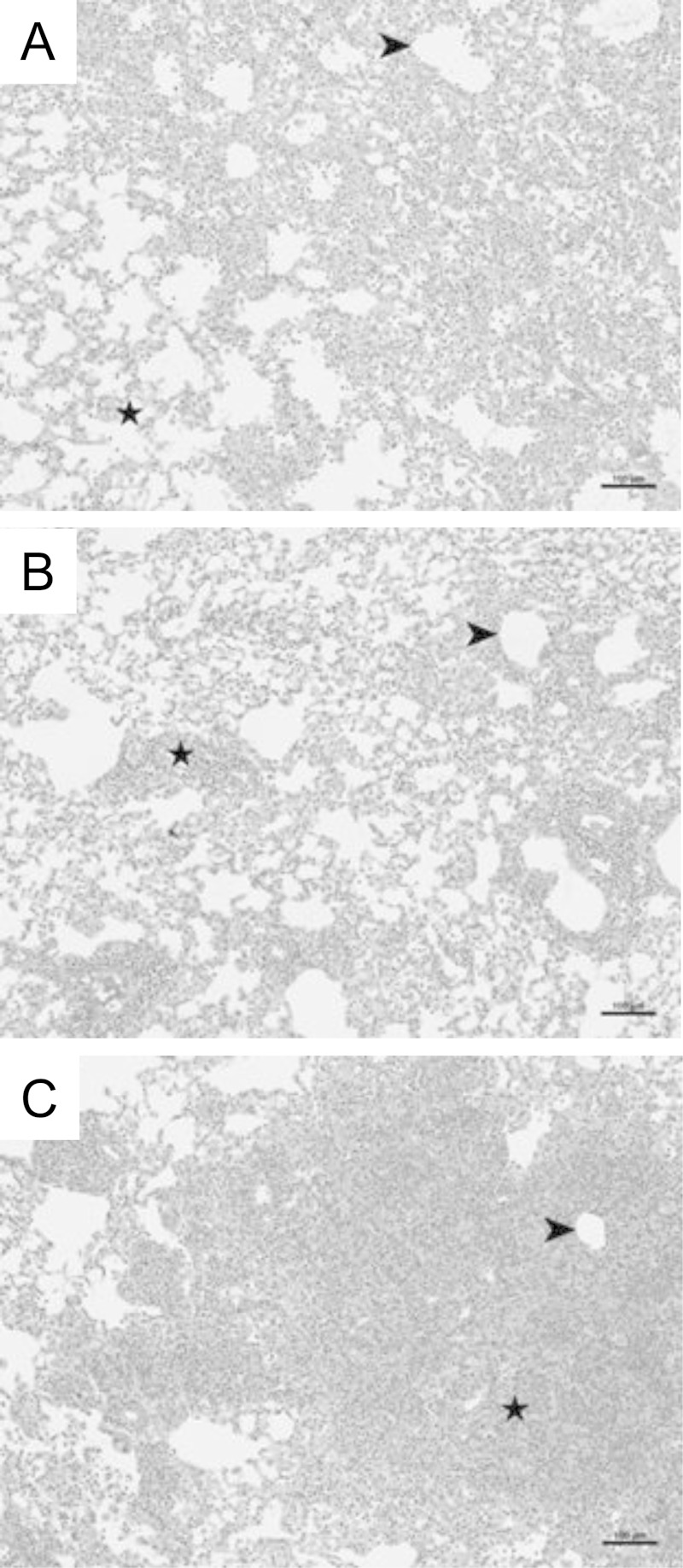
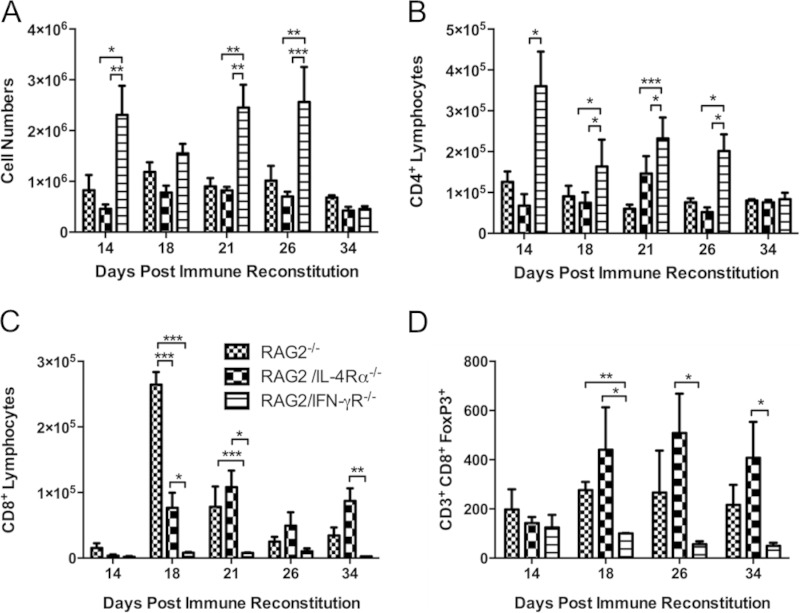
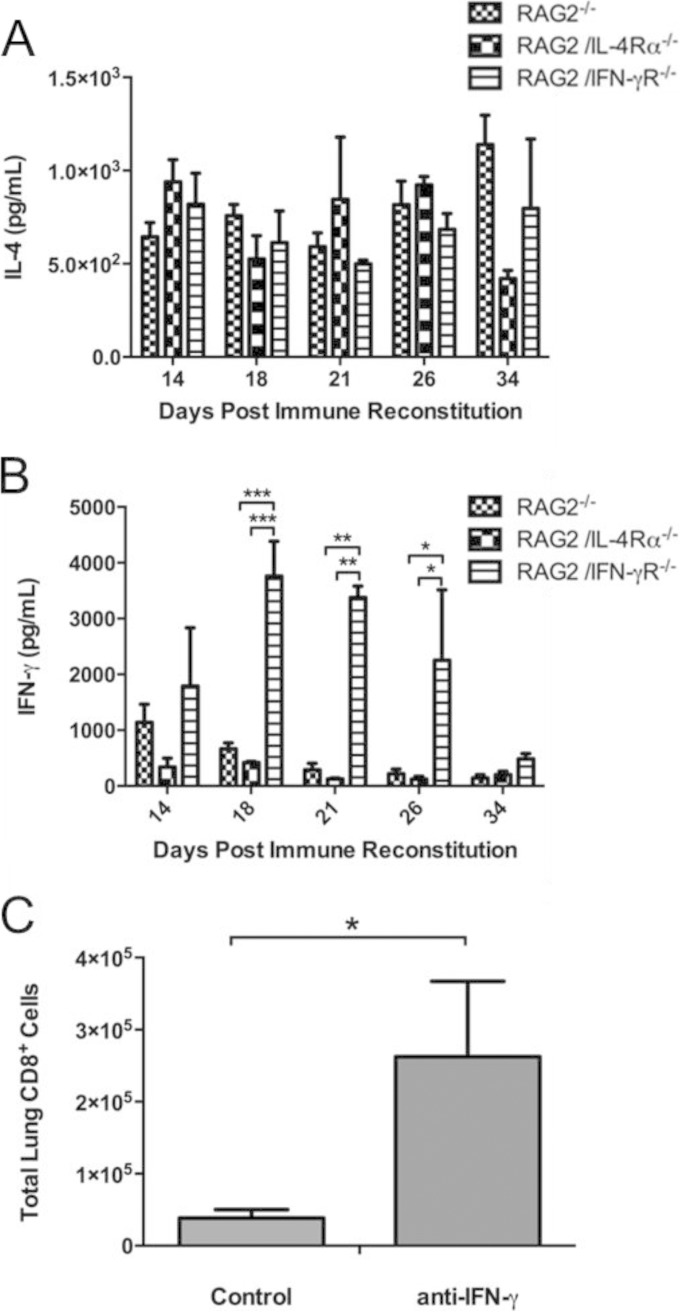
Pneumocystis is a respiratory fungal pathogen that causes pneumonia (Pneumocystis pneumonia [PcP]) in immunocompromised patients. Alveolar macrophages are critical effectors for CD4(+) T cell-dependent clearance of Pneumocystis, and previous studies found that alternative macrophage activation accelerates fungal clearance during PcP-related immune reconstitution inflammatory syndrome (IRIS). However, the requirement for either classically or alternatively activated macrophages for Pneumocystis clearance has not been determined. Therefore, RAG2(-/-) mice lacking either the interferon gamma (IFN-γ) receptor (IFN-γR) or interleukin 4 receptor alpha (IL-4Rα) were infected with Pneumocystis. These mice were then immune reconstituted with wild-type lymphocytes to preserve the normal T helper response while preventing downstream effects of Th1 or Th2 effector cytokines on macrophage polarization. As expected, RAG2(-/-) mice developed severe disease but effectively cleared Pneumocystis and resolved IRIS. Neither RAG/IFN-γR(-/-) nor RAG/IL-4Rα(-/-) mice displayed impaired Pneumocystis clearance. However, RAG/IFN-γR(-/-) mice developed a dysregulated immune response, with exacerbated IRIS and greater pulmonary function deficits than those in RAG2 and RAG/IL-4Rα(-/-) mice. RAG/IFN-γR(-/-) mice had elevated numbers of lung CD4(+) T cells, neutrophils, eosinophils, and NK cells but severely depressed numbers of lung CD8(+) T suppressor cells. Impaired lung CD8(+) T cell responses in RAG/IFN-γR(-/-) mice were associated with elevated lung IFN-γ levels, and neutralization of IFN-γ restored the CD8 response. These data demonstrate that restricting the ability of macrophages to polarize in response to Th1 or Th2 cytokines does not impair Pneumocystis clearance. However, a cell type-specific IFN-γ/IFN-γR-dependent mechanism regulates CD8(+) T suppressor cell recruitment, limits immunopathogenesis, preserves lung function, and enhances the resolution of PcP-related IRIS.
Copyright © 2015, American Society for Microbiology. All Rights Reserved.
Figures
Similar articles
-
Immune reconstitution inflammatory syndrome associated with pulmonary pathogens.Eur Respir Rev. 2017 Jan 3;26(143):160042. doi: 10.1183/16000617.0042-2016. Print 2017 Jan. Eur Respir Rev. 2017. PMID: 28049128 Free PMC article. Review.
-
The Dual Benefit of Sulfasalazine on Pneumocystis Pneumonia-Related Immunopathogenesis and Antifungal Host Defense Does Not Require IL-4Rα-Dependent Macrophage Polarization.Infect Immun. 2023 Apr 18;91(4):e0049022. doi: 10.1128/iai.00490-22. Epub 2023 Mar 14. Infect Immun. 2023. PMID: 36916933 Free PMC article.
-
Immune modulation with sulfasalazine attenuates immunopathogenesis but enhances macrophage-mediated fungal clearance during Pneumocystis pneumonia.PLoS Pathog. 2010 Aug 19;6(8):e1001058. doi: 10.1371/journal.ppat.1001058. PLoS Pathog. 2010. PMID: 20808846 Free PMC article.
-
Role of type I IFNs in pulmonary complications of Pneumocystis murina infection.J Immunol. 2005 May 1;174(9):5462-71. doi: 10.4049/jimmunol.174.9.5462. J Immunol. 2005. PMID: 15843544
-
Immunopathogenesis of Pneumocystis carinii pneumonia.Expert Rev Mol Med. 2005 Nov 14;7(26):1-16. doi: 10.1017/S1462399405010203. Expert Rev Mol Med. 2005. PMID: 16842636 Review.
Cited by
-
Understanding mechanisms underlying the pathology of immune reconstitution inflammatory syndrome (IRIS) by using animal models.Curr Clin Microbiol Rep. 2018 Sep;5(3):201-209. doi: 10.1007/s40588-018-0099-5. Epub 2018 Jun 22. Curr Clin Microbiol Rep. 2018. PMID: 30555775 Free PMC article.
-
Immune reconstitution inflammatory syndrome associated with Pneumocystis pneumonia in a patient with AIDS.J Int Med Res. 2020 Aug;48(8):300060520946544. doi: 10.1177/0300060520946544. J Int Med Res. 2020. PMID: 32851886 Free PMC article.
-
Intrinsic Programming of Alveolar Macrophages for Protective Antifungal Innate Immunity Against Pneumocystis Infection.Front Immunol. 2018 Sep 19;9:2131. doi: 10.3389/fimmu.2018.02131. eCollection 2018. Front Immunol. 2018. PMID: 30283457 Free PMC article.
-
Immune reconstitution inflammatory syndrome associated with pulmonary pathogens.Eur Respir Rev. 2017 Jan 3;26(143):160042. doi: 10.1183/16000617.0042-2016. Print 2017 Jan. Eur Respir Rev. 2017. PMID: 28049128 Free PMC article. Review.
-
Pneumocystis infection alters the activation state of pulmonary macrophages.Immunobiology. 2017 Feb;222(2):188-197. doi: 10.1016/j.imbio.2016.10.003. Epub 2016 Oct 5. Immunobiology. 2017. PMID: 27720434 Free PMC article.
References
-
- Hardak E, Oren I, Dann EJ, Yigla M, Faibish T, Rowe JM, Avivi I. 2012. The increased risk for Pneumocystis pneumonia in patients receiving rituximab-CHOP-14 can be prevented by the administration of trimethoprim/sulfamethoxazole: a single-center experience. Acta Haematol 127:110–114. doi:10.1159/000334113. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
