

Efficacy and Safety of Trabectedin or Dacarbazine for Metastatic Liposarcoma or Leiomyosarcoma After Failure of Conventional Chemotherapy: Results of a Phase III Randomized Multicenter Clinical Trial
- PMID: 26371143
- PMCID: PMC5070559
- DOI: 10.1200/JCO.2015.62.4734
Efficacy and Safety of Trabectedin or Dacarbazine for Metastatic Liposarcoma or Leiomyosarcoma After Failure of Conventional Chemotherapy: Results of a Phase III Randomized Multicenter Clinical Trial
Abstract
Purpose: This multicenter study, to our knowledge, is the first phase III trial to compare trabectedin versus dacarbazine in patients with advanced liposarcoma or leiomyosarcoma after prior therapy with an anthracycline and at least one additional systemic regimen.
Patients and methods: Patients were randomly assigned in a 2:1 ratio to receive trabectedin or dacarbazine intravenously every 3 weeks. The primary end point was overall survival (OS), secondary end points were disease control-progression-free survival (PFS), time to progression, objective response rate, and duration of response-as well as safety and patient-reported symptom scoring.
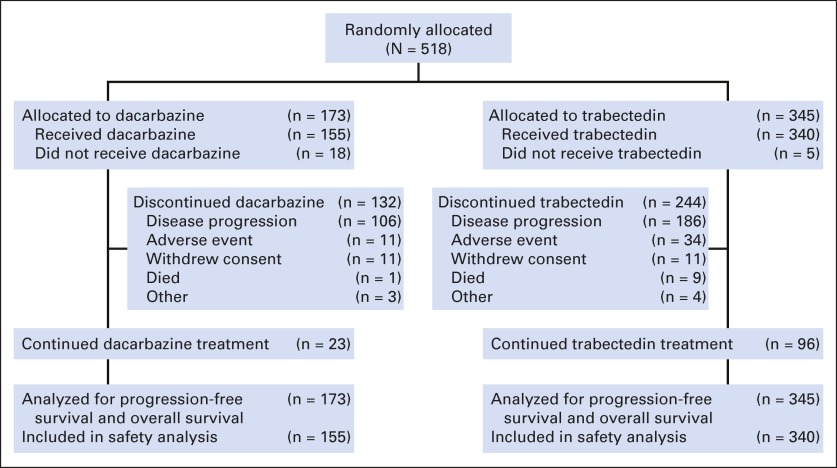
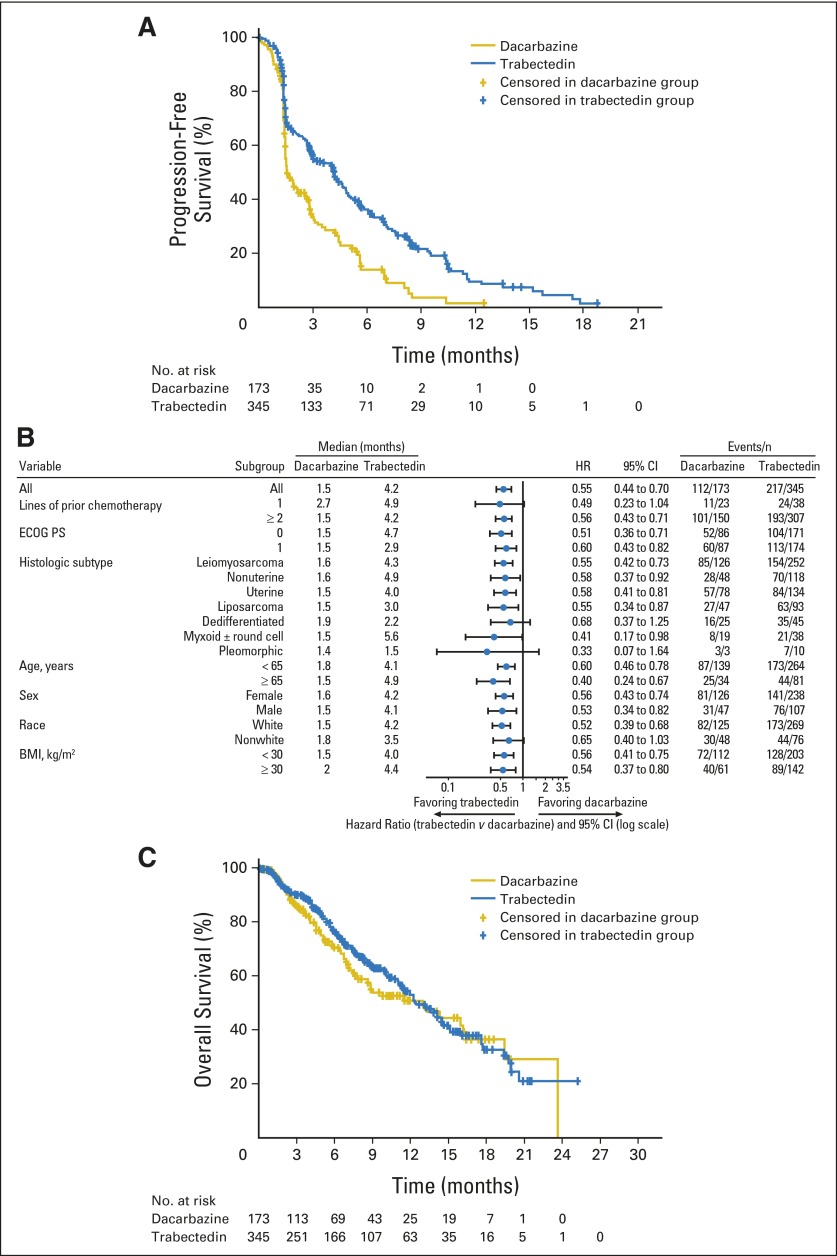
Results: A total of 518 patients were enrolled and randomly assigned to either trabectedin (n = 345) or dacarbazine (n = 173). In the final analysis of PFS, trabectedin administration resulted in a 45% reduction in the risk of disease progression or death compared with dacarbazine (median PFS for trabectedin v dacarbazine, 4.2 v 1.5 months; hazard ratio, 0.55; P < .001); benefits were observed across all preplanned subgroup analyses. The interim analysis of OS (64% censored) demonstrated a 13% reduction in risk of death in the trabectedin arm compared with dacarbazine (median OS for trabectedin v dacarbazine, 12.4 v 12.9 months; hazard ratio, 0.87; P = .37). The safety profiles were consistent with the well-characterized toxicities of both agents, and the most common grade 3 to 4 adverse effects were myelosuppression and transient elevation of transaminases in the trabectedin arm.
Conclusion: Trabectedin demonstrates superior disease control versus conventional dacarbazine in patients who have advanced liposarcoma and leiomyosarcoma after they experience failure of prior chemotherapy. Because disease control in advanced sarcomas is a clinically relevant end point, this study supports the activity of trabectedin for patients with these malignancies.
Trial registration: ClinicalTrials.gov NCT01343277.
© 2015 by American Society of Clinical Oncology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest are found in the article online at www.jco.org. Author contributions are found at the end of this article.
Figures
Comment in
-
Trabectedin and the L-Sarcomas: A Decade-Long Odyssey.J Clin Oncol. 2016 Mar 10;34(8):769-71. doi: 10.1200/JCO.2015.63.5938. Epub 2015 Sep 14. J Clin Oncol. 2016. PMID: 26371135 No abstract available.
-
Reply to S. Rastogi et al.J Clin Oncol. 2016 Oct 10;34(29):3583. doi: 10.1200/JCO.2016.68.3029. J Clin Oncol. 2016. PMID: 27458282 No abstract available.
-
Trabectedin in Soft Tissue Sarcoma: Have We Hit the Bull's-eye?J Clin Oncol. 2016 Oct 10;34(29):3582-3583. doi: 10.1200/JCO.2015.65.7130. J Clin Oncol. 2016. PMID: 27458287 No abstract available.
-
Reply to S. Rastogi et al.J Clin Oncol. 2016 Oct 10;34(29):3584. doi: 10.1200/JCO.2016.68.3037. J Clin Oncol. 2016. PMID: 27458303 No abstract available.
References
-
- Van Glabbeke M, van Oosterom AT, Oosterhuis JW, et al. Prognostic factors for the outcome of chemotherapy in advanced soft tissue sarcoma: An analysis of 2,185 patients treated with anthracycline-containing first-line regimens—A European Organization for Research and Treatment of Cancer Soft Tissue and Bone Sarcoma Group study. J Clin Oncol. 1999;17:150–157. - PubMed
-
- Clark MA, Fisher C, Judson I, et al. Soft-tissue sarcomas in adults. N Engl J Med. 2005;353:701–711. - PubMed
-
- Santoro A, Tursz T, Mouridsen H, et al. Doxorubicin versus CYVADIC versus doxorubicin plus ifosfamide in first-line treatment of advanced soft tissue sarcomas: A randomized study of the European Organization for Research and Treatment of Cancer Soft Tissue and Bone Sarcoma Group. J Clin Oncol. 1995;13:1537–1545. - PubMed
-
- Patel SR, Vadhan-Raj S, Burgess MA, et al. Results of two consecutive trials of dose-intensive chemotherapy with doxorubicin and ifosfamide in patients with sarcomas. Am J Clin Oncol. 1998;21:317–321. - PubMed
-
- Judson I, Verweij J, Gelderblom H, et al. Doxorubicin alone versus intensified doxorubicin plus ifosfamide for first-line treatment of advanced or metastatic soft-tissue sarcoma: A randomized controlled phase III trial. Lancet Oncol. 2014;15:415–423. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
