

A stepped-wedge evaluation of an initiative to spread the collaborative care model for depression in primary care
- PMID: 26371261
- PMCID: PMC4569448
- DOI: 10.1370/afm.1842
A stepped-wedge evaluation of an initiative to spread the collaborative care model for depression in primary care
Abstract
Purpose: Scale-up and spread of evidence-based practices is one of the most important challenges facing health care. We tested whether a statewide initiative, Depression Improvement Across Minnesota-Offering a New Direction (DIAMOND), to implement the collaborative care model for depression in 75 primary care clinics resulted in patient outcome improvements corresponding to those reported in randomized controlled trials.
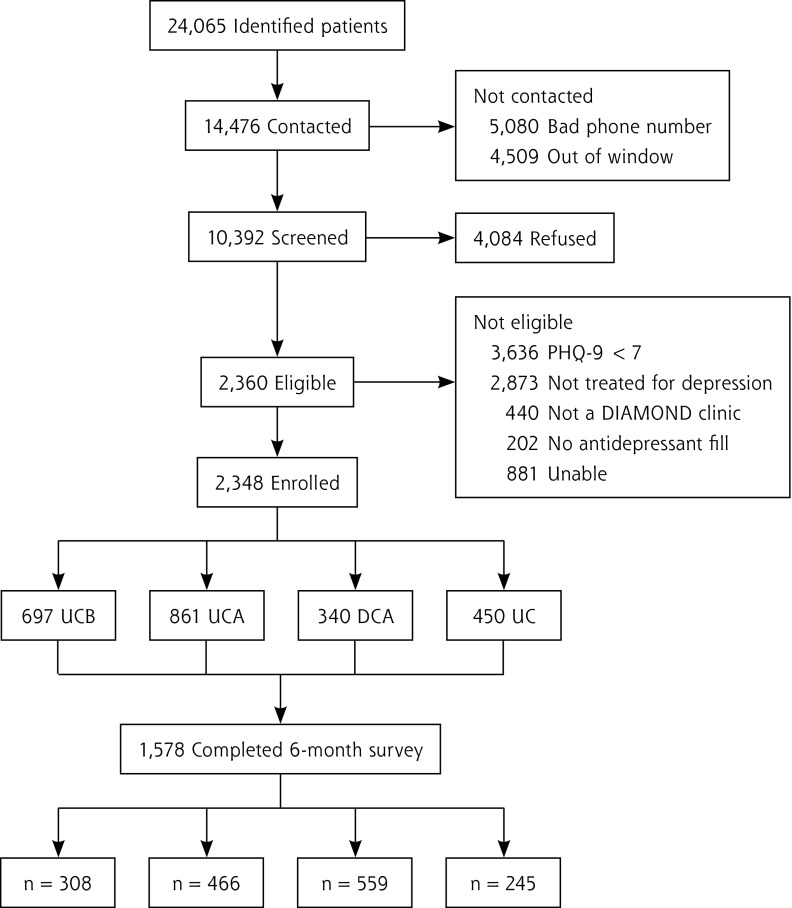
Methods: Health plans provided a new monthly payment to participating clinics after a 6-month intensive training program with ongoing data submission, networking, and consultation. Implementation was staggered, with 5 sequences of 10 to 40 clinics every 6 months. Payers provided weekly contact information for members from participating clinics who were filling antidepressant prescriptions, and we conducted baseline and 6-month surveys of 1,578 patients about their care and outcomes.
Results: There were 466 patients in DIAMOND clinics who received usual care before implementation (UCB), 559 who received usual care in DIAMOND clinics after implementation (UCA), 245 who received DIAMOND care after implementation (DCA), and 308 who received usual care in comparison clinics (UC). Patients who received DIAMOND care after implementation reported more collaborative care depression services than the 3 comparison groups (10.9 vs 6.4-6.7, on a scale of 0 of 14, where higher numbers indicate more services; P <.001) and more satisfaction with their care (4.0 vs 3.4 on a scale 1 to 5, in which higher scores indicate higher satisfaction; P ≤.001). Depression remission rates, however, were not significantly different among the 4 groups (36.4% DCA vs 35.8% UCB, 35.0% UCA, 33.9% UC; P = .94).
Conclusions: Despite the incentive of a supporting payment change and intensive training and support for clinics volunteering to participate, no difference in depression outcomes was documented. Specific unmeasured actions present in trials but not present in these clinics may be critical for successful outcome improvement.
Keywords: collaborative care; depression; health care delivery; primary care; quality.
© 2015 Annals of Family Medicine, Inc.
Figures
References
-
- Jacob V, Chattopadhyay SK, Sipe TA, Thota AB, Byard GJ, Chapman DP; Community Preventive Services Task Force. Economics of collaborative care for management of depressive disorders: a community guide systematic review. Am J Prev Med. 2012;42(5):539–549. - PubMed
-
- O’Connor EA, Whitlock EP, Beil TL, Gaynes BN. Screening for depression in adult patients in primary care settings: a systematic evidence review. Ann Intern Med. 2009;151(11):793–803. - PubMed
-
- Thota AB, Sipe TA, Byard GJ, et al. ; Community Preventive Services Task Force. Collaborative care to improve the management of depressive disorders: a community guide systematic review and meta-analysis. Am J Prev Med. 2012;42(5):525–538. - PubMed
-
- U.S. Preventive Services Task Force. Screening for depression in adults: U.S. preventive services task force recommendation statement. Ann Intern Med. 2009;151(11):784–792. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical