

Characterizing retention in HAART as a recurrent event process: insights into 'cascade churn'
- PMID: 26372279
- PMCID: PMC4571284
- DOI: 10.1097/QAD.0000000000000746
Characterizing retention in HAART as a recurrent event process: insights into 'cascade churn'
Abstract
Objective: The benefits of HAART rely on continuous lifelong treatment retention. We used linked population-level health administrative data to characterize durations of HAART retention and nonretention.
Design: This is a retrospective cohort study.
Methods: We considered individuals initiating HAART in British Columbia (1996-2012). An HAART episode was considered discontinued if individuals had a gap of at least 30 days between days in which medication was prescribed. We considered durations of HAART retention and nonretention separately, and used Cox proportional hazards frailty models to identify demographic and treatment-related factors associated with durations of HAART retention and nonretention.
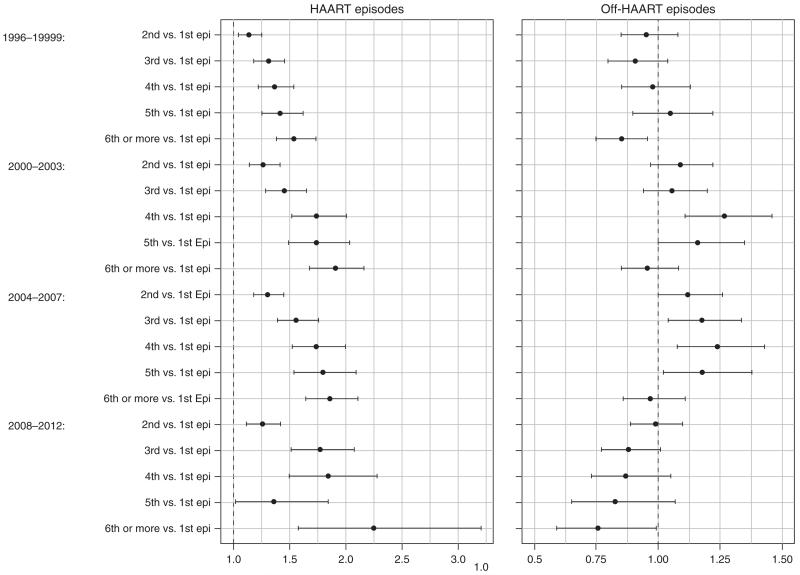
Results: Six thousand one hundred fifty-two individuals were included in the analysis; 81.2% were male, 40.6% were people who inject drugs, and 42.8% initiated treatment with CD4 cell count less than 200 cells/μl. Overall, 29% were continuously retained on HAART through the end of follow-up. HAART episodes were a median 6.8 months (25th, 75th percentile: 2.3, 19.5), whereas off-HAART episodes lasted a median 1.9 months (1.2, 4.5). In Cox proportional hazards frailty models, durations of HAART retention improved over time. Successive treatment episodes tended to decrease in duration among those with multiple attempts, whereas off-HAART episodes remained relatively stable. Younger age, earlier stages of disease progression, and injection drug use were all associated with shorter durations of HAART retention and longer off-HAART durations.
Conclusion: Metrics to monitor HAART retention, dropout, and reentry should be prioritized for HIV surveillance. Clinical strategies and public health policies are urgently needed to improve HAART retention, particularly among those at earlier stages of disease progression, the young, and people who inject drugs.
Figures
Similar articles
-
Non-medically supervised treatment interruptions among participants in a universally accessible antiretroviral therapy programme.HIV Med. 2010 May;11(5):299-307. doi: 10.1111/j.1468-1293.2009.00779.x. Epub 2009 Dec 8. HIV Med. 2010. PMID: 20002777
-
Initiating highly active antiretroviral therapy and continuity of HIV care: the impact of incarceration and prison release on adherence and HIV treatment outcomes.Antivir Ther. 2004 Oct;9(5):713-9. Antivir Ther. 2004. PMID: 15535408
-
Characterizing Human Immunodeficiency Virus Antiretroviral Therapy Interruption and Resulting Disease Progression Using Population-Level Data in British Columbia, 1996-2015.Clin Infect Dis. 2017 Oct 16;65(9):1496-1503. doi: 10.1093/cid/cix570. Clin Infect Dis. 2017. PMID: 29048508 Free PMC article.
-
Predictors of highly active antiretroviral therapy utilization for behaviorally HIV-1-infected youth: impact of adult versus pediatric clinical care site.J Adolesc Health. 2012 May;50(5):471-7. doi: 10.1016/j.jadohealth.2011.09.001. Epub 2011 Nov 4. J Adolesc Health. 2012. PMID: 22525110 Free PMC article.
-
Study of the impact of HIV genotypic drug resistance testing on therapy efficacy.Verh K Acad Geneeskd Belg. 2001;63(5):447-73. Verh K Acad Geneeskd Belg. 2001. PMID: 11813503 Review.
Cited by
-
Trends in HIV care cascade engagement among diagnosed people living with HIV in Ontario, Canada: A retrospective, population-based cohort study.PLoS One. 2019 Jan 4;14(1):e0210096. doi: 10.1371/journal.pone.0210096. eCollection 2019. PLoS One. 2019. PMID: 30608962 Free PMC article.
-
Cyclical Engagement in HIV Care: A Qualitative Study of Clinic Transfers to Re-enter HIV Care in Cape Town, South Africa.AIDS Behav. 2022 Jul;26(7):2387-2396. doi: 10.1007/s10461-022-03582-z. Epub 2022 Jan 21. AIDS Behav. 2022. PMID: 35061116 Free PMC article.
-
Behavioural, social and structural-level risk factors for developing AIDS among HIV-positive people who use injection drugs in a Canadian setting, 1996-2017.AIDS Care. 2020 Oct;32(10):1262-1267. doi: 10.1080/09540121.2020.1772955. Epub 2020 May 31. AIDS Care. 2020. PMID: 32476442 Free PMC article.
-
An Exploratory Study to Assess Individual and Structural Level Barriers Associated With Poor Retention and Re-engagement in Care Among Persons Living With HIV/AIDS.J Acquir Immune Defic Syndr. 2017 Feb 1;74 Suppl 2(Suppl 2):S113-S120. doi: 10.1097/QAI.0000000000001242. J Acquir Immune Defic Syndr. 2017. PMID: 28079721 Free PMC article.
-
Developing a triage tool for use in identifying people living with HIV who are at risk for non-retention in HIV care.Int J STD AIDS. 2020 Mar;31(3):244-253. doi: 10.1177/0956462419893538. Epub 2020 Feb 9. Int J STD AIDS. 2020. PMID: 32036751 Free PMC article.
References
-
- Carpenter CCJ, Fischl MA, Hammer SM, Hirsch MS, Jacobsen DM, Katzenstein DA, et al. Antiretroviral therapy for HIV infection in 1996 – recommendations of an international panel. J Am Med Assoc. 1996;276:146–154. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
